Cycle Readiness Decision Framework
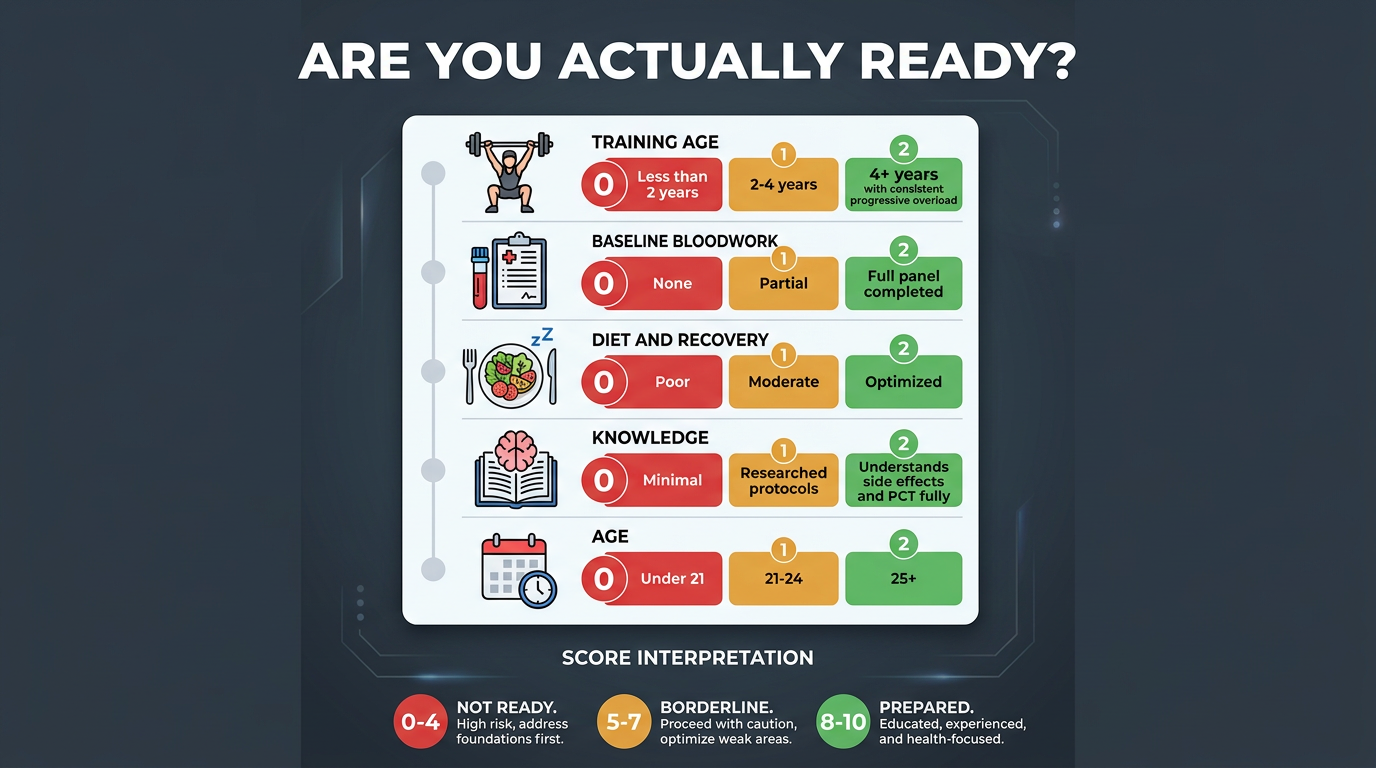
A clear-eyed decision framework covering age prerequisites, natural training ceiling, health requirements, psychological readiness, and the legitimate reasons to say no, at least for now.
- Evaluate whether you have reached your genetic potential through natural training
- Understand the physiological reasons behind age thresholds for anabolic compound use
- Identify health prerequisites and baseline bloodwork requirements
- Recognize psychological risk factors that make anabolic use higher-risk
- Know which conditions or circumstances make the answer categorically 'no' for now
The Question Nobody Asks Carefully Enough
Most people who start researching anabolic steroids spend their time asking which compounds to use, how much to take, and where to get them. Relatively few spend serious time asking whether they should do this at all, or whether this is the right moment in their life to make this decision. That omission is a mistake, and it produces outcomes ranging from disappointing to genuinely harmful. This lesson exists to give you the framework for honest self-assessment before you move on to the practical logistics.
This lesson is not meant to scare you away. Testosterone and related compounds, used intelligently by informed adults, carry manageable risks. It is meant to make sure that if and when you proceed, you do so with realistic expectations, appropriate preparation, and a genuine understanding of what you are trading off. The worst outcomes in this space come overwhelmingly from people who skipped this step.
Age: Why 25+ Is Not Just a Convention
The most commonly cited age threshold for beginning anabolic steroid use is 25. This is grounded in endocrine development, not moralizing. The hypothalamic-pituitary-gonadal axis, which governs natural testosterone production, is still undergoing final calibration through the mid-twenties for most men. The HPTA reaches its mature, stable setpoint somewhere in this range, after which baseline total testosterone and the feedback sensitivity of the system are essentially fixed.
Introducing exogenous androgens during this calibration phase creates a problem: suppression of endogenous production is a normal, predictable consequence of any anabolic cycle, and it may interfere with the axis during a period when it is still establishing its long-term functional baseline. A 19-year-old who runs a cycle and does PCT faces meaningfully higher odds of incomplete hormonal recovery than a 27-year-old doing the same thing, not because the compounds are categorically more dangerous, but because the target system is not finished developing.
There is also the question of the brain. Androgenic receptors are distributed throughout the central nervous system, and the prefrontal cortex continues maturing until approximately 25. Supraphysiological androgen exposure during this window has neurological implications that are less well-characterised than the endocrine risks but not trivially dismissible. The research on adolescent steroid use, while methodologically imperfect, consistently shows disruptions to mood regulation, impulsivity, and risk-assessment that do not fully reverse in some users.
None of this means that using Testosterone at 22 causes permanent harm in every case. Many thousands of men have done so without obvious lasting damage. But the margin for error is smaller, the physiological stakes are higher, and the potential benefit, more muscle at an age when natural gains are still abundant, is comparatively modest. The calculus genuinely does not favour it for most people under 23, and is still questionable for most people between 23 and 25 unless natural potential has been genuinely exhausted.
The Natural Training Ceiling
The most important non-age criterion is whether you have genuinely trained your natural genetic potential to a meaningful degree. Reaching theoretical maximum takes over a decade of optimal training for most people. The real question is whether you are in a position to learn anything from a cycle that you couldn’t learn without one.
A useful working benchmark: at minimum, three to four years of consistent, progressive, well-structured resistance training with adequate nutrition. For most men, this means approaching or exceeding rough natural strength standards, something in the range of a 1.5× bodyweight squat, 1.75× deadlift, 1.25× bench press is commonly cited as a reasonable marker of developed intermediate-to-advanced natural strength. More importantly, it means months of clear evidence that the primary limiting factor in your progress is no longer technique, consistency, or nutrition.
Why does this matter practically, beyond abstract principle? Because one of the most valuable functions of a first cycle is teaching you how your body responds to elevated androgens. You learn how you aromatize, how you recover, how your joints and tendons respond to rapid strength increases, how your skin reacts, how your sleep changes. If you do not yet have a strong baseline understanding of how your body responds to training stress, built from years of natural training, you have almost no framework for distinguishing cycle effects from confounders. The result is that you get less information from the cycle, and more of your decisions get made based on guesswork.
There is also a practical risk for underprepared trainees: anabolic compounds increase protein synthesis and nitrogen retention dramatically, which accelerates muscle and strength gains. Tendons and ligaments do not adapt at the same rate as muscle tissue, especially in the presence of supraphysiological androgens. A beginner whose tendons and joint capsules are not conditioned by years of progressive loading is meaningfully more likely to injure themselves when their muscle contractile force suddenly exceeds what their connective tissue has been built to support. Rotator cuff tears, bicep tendon ruptures, and patellar tendon issues are disproportionately common in undertrained users on their first cycle.
Honestly evaluate where you sit. If you have been training for two years and are still running a basic linear progression program, you are not at a natural plateau. You are at a training and consistency problem, and a cycle will not fix that. It will temporarily mask it.
Health Prerequisites: Bloodwork Before You Consider Anything
No responsible discussion of beginning a cycle omits bloodwork. You need a baseline panel before you ever touch a compound, and the results of that panel are part of the go/no-go decision, not an afterthought to satisfy at some later stage.
The minimum baseline panel should include: total testosterone and free testosterone, SHBG, estradiol (sensitive assay), LH and FSH, prolactin, a complete blood count with particular attention to hematocrit and hemoglobin, a full lipids panel (fasted), liver enzymes (ALT, AST, GGT), comprehensive metabolic panel (kidney function, glucose), and blood pressure measured across multiple readings over several days. If you are over 35 or have a family history of prostate disease, add PSA.
Why does this matter for the decision? Because this panel may reveal conditions that either contraindicate the use of exogenous androgens entirely or that substantially change the risk calculus. A man with a baseline hematocrit of 48% is already near the upper end of normal, androgen use will push him into ranges associated with significantly elevated cardiovascular risk. A man with a natural total testosterone of 800 ng/dL and no symptoms of deficiency is trading a genuinely normal hormonal environment for a supraphysiological one; the case for benefits over risks looks very different for him than for a man with a baseline of 300 ng/dL. A man with HDL of 28 mg/dL before touching a compound is already running a serious lipid disadvantage; any cycle will worsen this.
Beyond compound-specific interactions, baseline bloodwork identifies pre-existing conditions. Elevated PSA, kidney disease, elevated liver enzymes from non-alcoholic fatty liver, polycythemia, all of these are relevant pre-existing risk factors. You cannot make an informed decision about adding exogenous hormones to an unknown physiological baseline.
Psychological Readiness: The Factor Most People Skip
Psychological readiness is the least discussed and arguably most important dimension of this decision. The body image and self-perception dynamics of physique-focused anabolic use are genuinely complex, and they interact with outcomes in ways that are not always predictable.
A clear warning sign is cycle initiation driven primarily by body dysmorphia, the persistent perception that one is inadequate, too small, or insufficiently lean despite objective evidence to the contrary. Body dysmorphic disorder (BDD) and its milder variants are significantly overrepresented in physique sport and in the population of people who research anabolic compounds. The problem is structural: exogenous androgens produce real physical changes, and those changes produce temporary satisfaction, but in the context of dysmorphia, the goalposts move. The new physique becomes the new baseline, the new dissatisfaction emerges, and the escalation logic, more compounds, higher doses, indefinitely, is built into the dynamic from the start.
If you find yourself unable to be in a social setting, obsessively tracking your appearance multiple times per day, experiencing significant distress about your physique despite being objectively athletic, or deriving your entire sense of self-worth from your physical appearance, these are signals that warrant addressing before adding hormonal compounds to the equation. Anabolic use will not fix these patterns, and it often accelerates them.
A realistic expectation calibration is also important. First cycles on Testosterone alone will produce meaningful but not cinematic results for most people. Expect 10–15 lb of retained lean mass gain after water weight normalises post-cycle, with significant individual variation. Expect strength to increase substantially. Do not expect to look like a professional bodybuilder. Do not expect results to be permanent without continued training and nutrition discipline. The degree of mismatch between expectations and results is one of the primary predictors of escalation into more aggressive, higher-risk protocols.
Legal and Practical Context
In most countries where this platform is likely accessed, the United States, Canada, the United Kingdom, Australia, anabolic steroids are scheduled controlled substances. Possession may be legal in some jurisdictions for personal use but illegal to supply; in others, simple possession is criminal. These are facts you should know before making a decision.
Practically, this means your supply chain has no quality control, no labelling standards, and no accountability mechanisms. Compounds obtained from underground laboratory sources may be underdosed, overdosed, contaminated, or mislabelled. Research suppliers carefully, verify third-party testing if possible, and approach your first cycle with the recognition that you are working with a degree of uncertainty about what is actually in the vial. Source quality research is a real and important part of preparation.
“Doing your research” genuinely means: reading primary literature on the compounds, not just forum anecdotes; understanding the pharmacokinetics before you begin; having a complete cycle plan including PCT before you start the cycle, not figuring it out midway; having Tamoxifen or Clomiphene on hand before your first injection, not ordering it in week eight; and having arranged your bloodwork before and during the cycle, not improvising it reactively when symptoms appear.
The Off-Ramp: When the Answer Is Categorically No Right Now
There are conditions under which the honest answer to “should I do this?” is not “proceed cautiously” but “no, not now.” These are not edge cases.
You are under 23. The endocrine and neurological development arguments are strongest in this range. Come back at 25 with a better foundation.
You have fewer than 3 years of serious, consistent training. You have too much natural potential remaining and insufficient physiological conditioning for the connective tissue demands of accelerated hypertrophy. The risk-benefit ratio doesn’t favour it.
You have not completed a baseline blood panel. You have no informed basis for a risk-benefit decision without knowing your starting point. This is non-negotiable.
Your bloodwork shows significant pre-existing abnormalities. Elevated hematocrit at baseline, severely depressed lipids, elevated liver enzymes, existing kidney disease, uncontrolled blood pressure, these are contraindications or require medical consultation before proceeding.
You do not have PCT compounds on hand and arranged before starting. Suppression of the HPTA is a certainty. A certainty, not a risk. Running a cycle without a concrete, purchased PCT plan is choosing to leave your hormonal recovery to chance.
You are in a period of significant mental health instability. Exogenous androgens modulate mood, aggression, and emotional regulation. Introducing them into an already dysregulated psychological state creates compounding risk.
You are in an active competition season in a tested sport, or employed in a profession that tests. This is obvious, but worth stating explicitly.
None of these off-ramps are permanent for most people. They are invitations to address the specific deficiency, then revisit the decision from a more informed position. The goal of this lesson is to ensure that if and when you use anabolic compounds, you are genuinely ready.
Selected references for major clinical, mechanistic, or protocol claims. Community-practice points may not be cited individually.