PCT Physiology, Timing, and SERM Protocols
Everything beginners need to know about Post-Cycle Therapy, the physiology of suppression, SERM protocols, timing based on ester half-life, recovery bloodwork, and the blast-and-cruise alternative.
- Explain what HPTA suppression means physiologically and why it doesn't resolve on its own
- Know the mechanism differences between Tamoxifen and Clomiphene and their standard PCT protocols
- Calculate correct PCT start timing based on ester half-life
- Use bloodwork to confirm genuine hormonal recovery
- Understand blast-and-cruise as an alternative for those choosing not to recover
How Suppression Works
Suppression of the HPTA is not a side effect in the usual sense, it is a direct, expected, dose-dependent physiological consequence of introducing exogenous androgens. Understanding the mechanism helps demystify why recovery does not happen on its own and why PCT is not optional.
The HPTA, the Hypothalamic-Pituitary-Testicular Axis, is the regulatory loop governing natural testosterone production. The hypothalamus produces GnRH (gonadotropin-releasing hormone), which signals the pituitary to release LH and FSH. LH signals the Leydig cells in the testes to produce testosterone; FSH stimulates spermatogenesis. Estradiol and testosterone, produced as a result, feed back to the hypothalamus and pituitary to down-regulate GnRH, LH, and FSH when levels are sufficient, a classic negative feedback loop.
When you introduce exogenous Testosterone at supraphysiological doses, circulating testosterone and estradiol (from aromatization) are both elevated dramatically. The hypothalamus and pituitary read these levels and, following normal negative feedback logic, suppress GnRH, LH, and FSH output toward zero. The testes receive no LH signal, and endogenous testosterone production falls to near-zero. The testes also begin to atrophy modestly from disuse, Leydig cell activity suppresses, and testicular volume may decrease noticeably (by 10–30% in many users on extended cycles). This is normal, expected, and fully reversible in the vast majority of cases with appropriate PCT.
The problem is that suppression does not resolve on its own immediately when you stop using the compound. The HPTA does not snap back the moment exogenous levels fall. The axis has been dormant, in some cases for 12–20 weeks, and restoring normal pulsatile GnRH and gonadotropin secretion requires time and, typically, targeted pharmacological stimulus. Without PCT, the restoration can take many months, during which time total testosterone may sit at low or low-normal levels, producing the classic post-cycle symptoms: fatigue, low libido, mood depression, strength loss, and difficulty retaining cycle gains.
Tamoxifen vs. Clomiphene: The Two SERM Options
PCT uses SERMs, Selective Estrogen Receptor Modulators, to restart HPTA function. The mechanism is elegant: SERMs block oestrogen receptors in the hypothalamus and pituitary, which removes the estradiol-mediated inhibitory signal and prompts a rebound increase in GnRH, LH, and FSH. Rising LH then stimulates the testes to resume testosterone production.
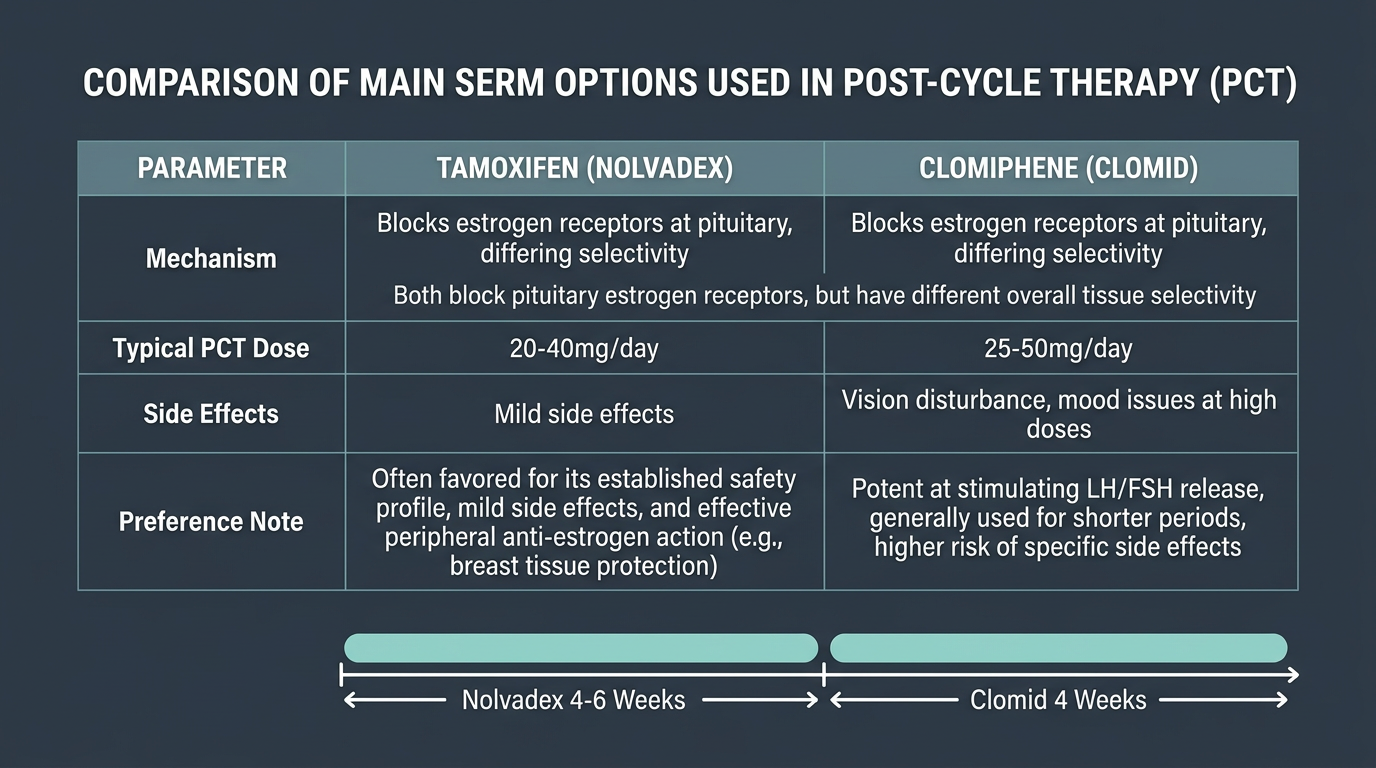
Tamoxifen (brand name Nolvadex) and Clomiphene (Clomid) are the two standard SERMs used in PCT. Both work through the same oestrogen-receptor blockade mechanism, but they differ in selectivity, potency, and side effect profiles in ways that matter practically.
Tamoxifen is selective in its action, it blocks oestrogen receptors in hypothalamic-pituitary tissue and breast tissue, but acts as an oestrogen agonist in other tissues (bone, lipid metabolism). In male PCT context, this selectivity is generally advantageous. Tamoxifen is effective, well-tolerated, and the incidence of significant side effects at PCT doses is relatively low. The standard PCT protocol is 20 mg/day for 6 weeks, or 40 mg/day for 4 weeks in some protocols, the higher dose for the first 1–2 weeks followed by 20 mg/day is also commonly used (40/40/20/20 or similar).
Clomiphene is more potent at hypothalamic stimulation and has a longer history in clinical male hypogonadism treatment. However, it is associated with a higher incidence of side effects at PCT doses, visual disturbances (halos, blurring), emotional volatility, and a quality sometimes described as a “dark” mood or dysphoria. These side effects are dose-related, and some users tolerate 25 mg/day reasonably well while finding 50 mg/day unpleasant. Standard Clomiphene PCT protocol: 25–50 mg/day for 4–6 weeks. Many practitioners now use Clomiphene at lower doses (25 mg/day) rather than the older 50 mg/day recommendation to reduce side effects while maintaining efficacy.
Combination PCT: Running Tamoxifen and Clomiphene together is a common protocol that many users find more effective than either alone, particularly after longer or heavier cycles. Tamoxifen 20 mg + Clomiphene 25 mg daily for 6 weeks is a frequently cited combination. The rationale is that they act on slightly different receptor populations and combining them provides broader axis stimulation.
For a beginner’s first PCT: Tamoxifen alone at 20–40 mg/day for 4–6 weeks is a well-supported, lower-risk starting protocol for a standard 10–16 week testosterone-only cycle. It is effective, well-tolerated, and sufficient for most first-cycle recovery scenarios. Add Clomiphene at 25 mg/day if you want belt-and-suspenders coverage, or if mid-cycle bloodwork indicated particularly deep suppression.
PCT Timing: When to Start Based on Ester Half-Life

Starting PCT too early is one of the most common and consequential beginner mistakes. If significant exogenous testosterone is still circulating, LH and FSH will be suppressed regardless of what SERM you are taking. The SERM cannot overcome the negative feedback signal of still-elevated testosterone and estradiol, beginning PCT with exogenous compound still on board wastes the SERM and fails to initiate meaningful HPTA recovery.
The rule is straightforward: wait approximately 5 half-lifes from your last injection before starting PCT. This allows exogenous compound levels to fall to a point low enough that the SERM's block on hypothalamic-pituitary estradiol receptors can produce meaningful rises in GnRH and gonadotropins.
For Testosterone Enanthate and Cypionate (both with half-lifes of approximately 7–9 days): in practice, most sources recommend starting PCT 14–18 days after the last injection of long-ester testosterone. This is a pragmatic compromise that accepts some residual circulating compound in exchange for not spending 6 weeks in the testosterone/estradiol trough before PCT begins. Levels at 14–18 days post-last-injection are well below saturation, and most SERM protocols are effective at this timing.
For Testosterone Propionate (half-life ~2–3 days): wait 4–7 days after last injection before starting PCT.
For Nandrolone Decanoate (half-life ~11–14 days): the long ester creates a specific complication. Many practitioners recommend waiting 3–4 weeks after the last Nandrolone Decanoate injection before PCT, which often means planning cycles with Deca ending 4 weeks before the testosterone does, or planning a longer post-cycle wait. Failing to account for [Nandrolone]'s long half-life in PCT timing is a known cause of poor recovery in Deca-containing cycles.
Duration of PCT and Bloodwork to Confirm Recovery
The duration of PCT is commonly 4–6 weeks. Shorter cycles (10–12 weeks) in most users achieve adequate HPTA restart in 4 weeks of PCT. Longer or heavier cycles (16 weeks+, higher doses) may warrant 6 weeks. There is no universal fixed timeline, the endpoint of PCT is not simply completing the weeks of SERM administration, but demonstrating hormonal recovery through bloodwork.
The recovery bloodwork draw should be done approximately 4 weeks after completing PCT (not during PCT, when the SERM itself is modifying LH and FSH dynamics). This timing, roughly 8–10 weeks after the last injection for a standard long-ester cycle, provides a clear read on where the HPTA has landed without pharmacological support.
Recovery targets: total testosterone returned to your personal baseline (ideally within 20% of your pre-cycle level), LH and FSH both above 1.0 IU/L and ideally returning toward your pre-cycle levels, estradiol normalised. If by 8–10 weeks post-cycle the HPTA has not meaningfully recovered, total testosterone below 300–400 ng/dL, LH/FSH still suppressed, that warrants medical evaluation by an endocrinologist or men’s health physician.
Blast-and-Cruise: Understanding the Alternative
Blast and cruise is the practice of never running PCT and never returning to natural testosterone levels, instead, alternating periods of supraphysiological compound use (blast) with periods of lower-dose testosterone maintenance typically approximating TRT replacement dosing (cruise). Standard cruise doses are 100–150 mg/week of Testosterone Enanthate or Cypionate, enough to maintain normal-to-low-normal physiological levels without the supraphysiological stimulus of the blast phase.
The explicit trade-off in blast and cruise is permanent HPTA suppression. Gonads are suppressed continuously and may not recover natural function at all after extended blast and cruise use. This is an accepted, known consequence of exogenous androgen use. Users who adopt blast and cruise are, in effect, choosing to become dependent on exogenous testosterone indefinitely, with the understanding that their natural production may not recover if they stop.
For this reason, blast and cruise is not a beginner decision, and arriving at it by default because PCT feels inconvenient is the wrong reason. It is a considered, deliberate choice made by experienced users who have a clear framework for managing TRT, have medical oversight, and have accepted the long-term implications. For a first-cycle beginner, the default should be PCT with full hormonal recovery.
Signs of Poor Recovery and When to Seek Medical Assessment
Poor PCT recovery manifests as persistent symptoms at 8+ weeks post-PCT: low libido, fatigue, mood depression, difficulty retaining strength or muscle, and, most importantly, bloodwork showing total testosterone below 350–400 ng/dL with still-suppressed LH and FSH. Slower recovery is common, particularly after longer or heavier cycles or when PCT timing was suboptimal.
If recovery bloodwork at 8–12 weeks post-cycle shows inadequate recovery, a second, longer PCT course may help. Persistent failure to recover, total testosterone below 300 ng/dL at 16+ weeks post-cycle with low gonadotropins, warrants endocrinology referral. Indefinite self-management with anecdotal protocols is not an adequate response here. A physician can evaluate for secondary hypogonadism, rule out structural pituitary issues (rare but real), and discuss treatment options including monitored TRT if the axis does not recover.
Selected references for major clinical, mechanistic, or protocol claims. Community-practice points may not be cited individually.