Common First-Cycle Side Effects
Practical management of the most frequent first-cycle side effects, acne, hair loss, sleep disruption, mood changes, water retention, and injection site issues, with clear severity grading and response frameworks.
- Identify and manage cycle-related acne at each severity grade
- Understand androgenic alopecia risk and the tradeoffs of finasteride use
- Recognise sleep disruption and night sweats as common cycle phenomena
- Distinguish hormonally-driven mood changes from personal baseline
- Know the difference between estrogen-driven water retention and injection site problems requiring medical attention
Acne: The Most Common Side Effect Nobody Fully Prepares For
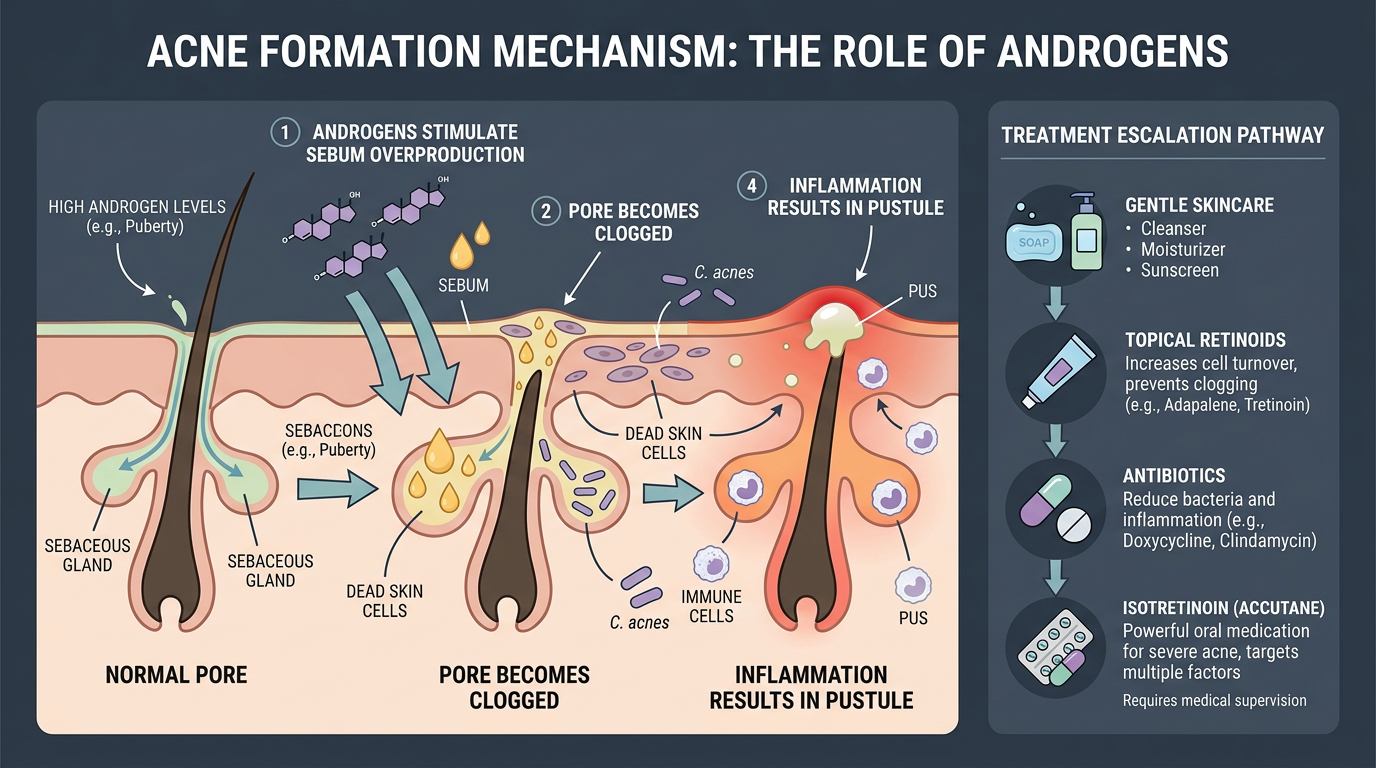
Acne is the most frequently encountered side effect of testosterone and anabolic steroid use, and it is also one of the most psychologically impactful, particularly when it moves beyond the face to affect the back, chest, and shoulders. Understanding why it happens and having a tiered management approach prepared before the cycle starts is significantly better than improvising reactively when breakouts appear.
The mechanism is androgenic: sebaceous glands express androgenic receptors, and elevated androgens, both directly (testosterone, DHT) and through DHT conversion via the 5AR enzyme, increase sebum (skin oil) production. Elevated sebum combined with accelerated skin cell turnover creates the conditions for pore blockage and the Propionibacterium acnes proliferation that produces inflammatory lesions. Individual susceptibility varies enormously based on genetics, some users run 600 mg/week of Testosterone with entirely clear skin; others break out at 300 mg/week in their first month.
A tiered management framework applies to severity grades. At grade 1 (mild, comedones and small papules): benzoyl peroxide wash (5–10%) used daily or twice daily, combined with salicylic acid toner. Clean pillowcases frequently. Avoid touching the face. Moderate dietary changes (reducing high-glycemic foods and dairy has some evidence). This level of acne is extremely common and manageable without prescription intervention.
At grade 2 (moderate, inflammatory papules and pustules): add topical retinoid (tretinoin 0.025–0.05% nightly) and topical clindamycin antibiotic. These require a prescription in most countries but are obtainable via telemedicine. This combination addresses sebum production (retinoid), bacterial load (clindamycin), and accelerates cell turnover. Allow 6–8 weeks for meaningful improvement with topical regimens.
At grade 3–4 (severe, cystic, back or chest involvement): oral antibiotics (doxycycline 100 mg twice daily for 6–12 weeks) combined with topical treatment. Consider whether the current compound dose or selection is appropriate. Isotretinoin (Accutane) is the nuclear option for cystic acne but creates significant drug interactions, teratogenicity, and requires close medical monitoring. Do not self-administer isotretinoin.
Compound selection matters for acne-prone individuals. DHT-derivative compounds, including Masteron, Anavar, Winstrol, and Trenbolone, are generally more acne-inducing for predisposed individuals because DHT itself is a potent activator of sebaceous glands. Nandrolone-based compounds ([Nandrolone] converts to DHN via 5AR rather than DHT, which has lower sebaceous receptor affinity) are often reported as less acne-causing by users. The trend is genuine in both anecdotal and mechanistic literature, though individual responses vary.
Hair Loss: The Androgenic Trade-Off You Need to Understand Before You Start
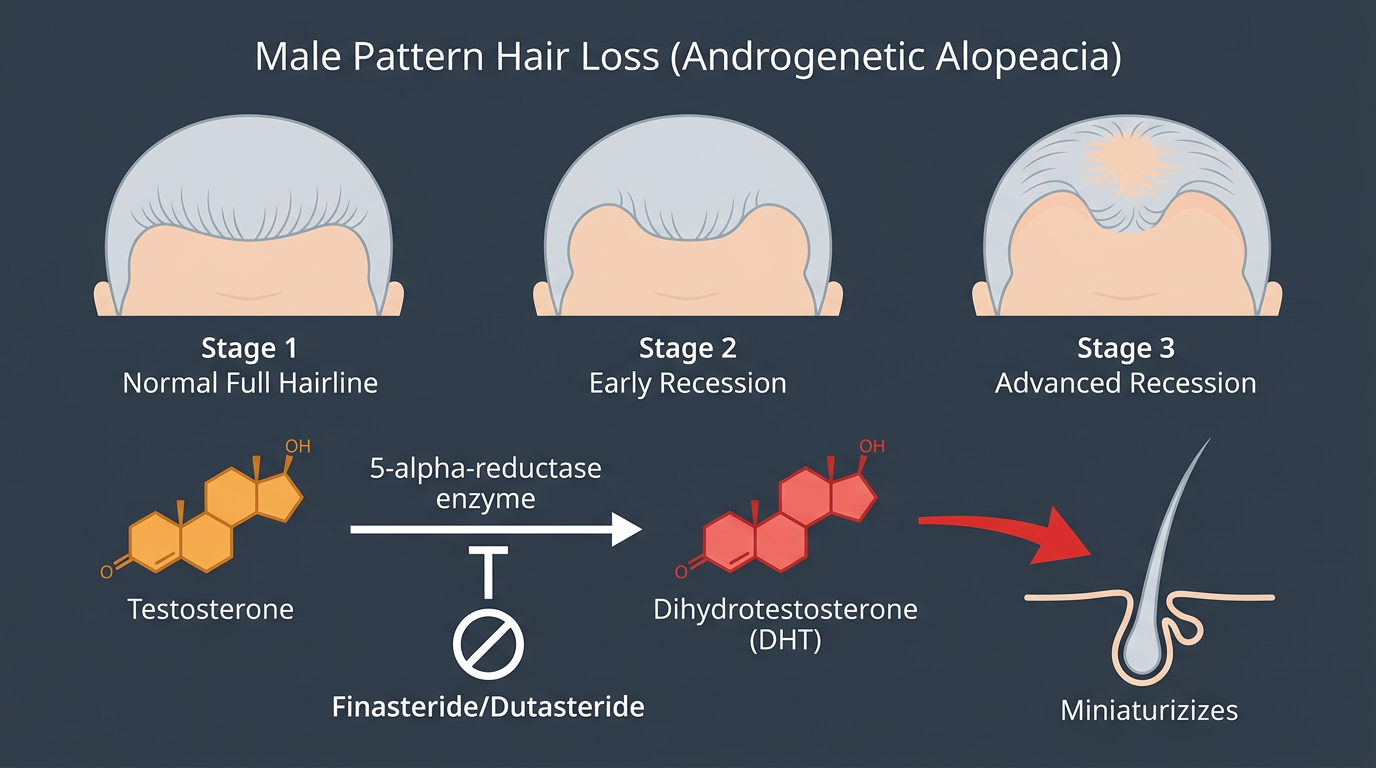
Androgenic alopecia (male pattern baldness) is genetically programmed in predisposed men, the hair follicles at the temples and crown contain androgenic receptors that, when activated by DHT, miniaturise and eventually cease producing terminal hair. Exogenous testosterone dramatically elevates both total testosterone and its DHT conversion product via the 5AR enzyme, accelerating this process in genetically predisposed individuals.
The critical point here: anabolic steroids do not cause hair loss in men who are not genetically predisposed to it. They accelerate the timeline in men who were going to lose their hair anyway. A man with no family history of male pattern baldness running 500 mg/week of Testosterone is unlikely to develop meaningful hairline recession from the cycle. A man with a strong family history who is already showing temporal recession at 25 is likely to experience meaningful acceleration.
Finasteride is a 5AR inhibitor that blocks the conversion of testosterone to DHT. At 1 mg/day (the standard hair loss dose), it reduces scalp and serum DHT by approximately 60–70%. This meaningfully attenuates the androgenic stimulus to follicles that drives accelerated shedding. However, it comes with trade-offs that beginners often underestimate.
Finasteride reduces serum DHT across the board, not just in the scalp. DHT plays a role in libido, erection quality, and certain aspects of mood and drive. Some users report measurable decreases in libido and erection quality on Finasteride; a minority report persistent sexual side effects even after cessation (post-finasteride syndrome, though this remains contested in the literature). Using Finasteride during a cycle also impairs the ability to manage DHT-mediated side effects by proxy, if your DHT is suppressed, it is harder to diagnose what is causing issues.
More practically for cycle planning: Finasteride does not protect against hair loss from DHT-derivative compounds. Masteron, Anavar, Winstrol, and Trenbolone are already DHT derivatives or have high androgenic receptor affinity without depending on 5AR conversion, they act directly. Finasteride blocks the conversion pathway (testosterone → DHT) but cannot reduce the activity of compounds that arrive at the androgen receptor without needing that conversion. Using Finasteride to “protect” your hair while stacking DHT derivatives is a common misunderstanding that does not work.
The honest advice for hair-loss-concerned beginners: assess your genetic risk honestly (look at your father and maternal grandfather), stick to compounds with lower androgenic potential on your first cycle (Testosterone is better than stacking DHT derivatives), and make a considered decision about Finasteride with an awareness of both its benefits and real risks.
Sleep Disruption and Night Sweats
Sleep disturbance is a frequently reported but often overlooked first-cycle side effect. The presentation varies, some users report difficulty initiating sleep, others report waking in the early morning hours, and many report night sweats significant enough to disrupt sleep.
Night sweats on a testosterone cycle are primarily a thermoregulatory effect. Elevated androgens increase basal metabolic rate and alter central temperature set points. The body’s nocturnal thermoregulation is disrupted, producing episodes of sweating during sleep that can range from mild dampness to sheets-and-pillow-soaking episodes. Trenbolone is particularly notorious for severe night sweats, more so than Testosterone alone, but the phenomenon occurs with many anabolic compounds.
Practical management: lower bedroom temperature, breathable bedding, wicking sleepwear, and ensuring estradiol is not excessively elevated (high estradiol worsens night sweats). Some users find timing their injections away from bedtime helps slightly. There is no pharmacological solution for this; it resolves after the cycle ends.
Sleep quality disruption beyond sweating, particularly reduced deep sleep and REM, is less consistently reported but does occur. Elevated androgens can alter cortisol rhythms and circadian signalling. If sleep quality is substantially impaired, this feeds into recovery and performance, which negates some of the cycle benefit. Maintaining good sleep hygiene (consistent sleep/wake times, dark room, no screens before bed) becomes more important, not less, during an active cycle.
Mood and Aggression: Distinguishing Hormonal Cause from Baseline
The relationship between anabolic compounds and mood is real, complex, and highly individual. The popular narrative of roid rage, explosive, uncontrolled aggression as a universal feature of steroid use, is substantially exaggerated in media and substantially underappreciated in community culture. The actual mood effects of testosterone at beginner doses are usually more subtle: increased assertiveness, reduced tolerance for frustration, somewhat heightened irritability under stress, and in some users, a notable increase in competitive drive. None of these are inherently problematic.
Where problems emerge is in users who had pre-existing mood regulation difficulties, anxiety, depression, anger management challenges, before beginning a cycle. Exogenous androgens do not create character traits that were not present before; they amplify tendencies that already exist and reduce the emotional buffering that normally modulates them. A person with a history of anger management challenges is likely to find their baseline worsened on a high-androgen cycle. A person with baseline anxiety may find estradiol fluctuations produce significant emotional volatility.
A useful frame for self-assessment during a cycle: ask yourself whether the reaction you are having to a situation is proportionate to what you would have experienced before the cycle, in the same scenario. If yes, the cycle is not driving it. If you find yourself having significantly disproportionate emotional responses, especially to interpersonal situations that would not previously have produced the same reaction, recognise that as a potential hormonal effect and engage the coping strategies you would use for any emotionally dysregulated state.
Estradiol management is often the most important lever for mood. Both high and crashed estradiol produce mood effects, the former characterised by emotional volatility and sensitivity, the latter by a flat, depressed, or anhedonic quality. If mood disturbance appears mid-cycle, bloodwork is the first diagnostic step.
Water Retention: Estrogen-Driven vs. Compound-Specific
Water retention is among the most commonly misunderstood side effects of beginner testosterone cycles. The soft, smooth, bloated appearance that many beginners notice in weeks 4–8 is overwhelmingly driven by estradiol-mediated sodium and water retention. As estradiol rises with increasing testosterone and aromatization, the kidneys retain more sodium through multiple mechanisms, and water follows. The result is increased extracellular fluid, visible as a puffier face, less defined waist, and a general “wet” appearance.
Managing this effectively comes back to estradiol control through appropriate (not excessive) AI use, confirmed with bloodwork. Dietary sodium restriction helps at the margin but does not address the root cause. Diuretics are occasionally used by competitive bodybuilders to address this acutely but have no place in a beginner health-maintenance framework.
It is important to distinguish estradiol-driven water retention from compound-specific water retention. Some compounds, particularly Nandrolone (Deca), produce water retention through mechanisms partly independent of estradiol, [Nandrolone] is a weak progesterone agonist and has glucocorticoid receptor activity that contributes to fluid retention. Managing estradiol alone may not fully address Nandrolone-related retention. This is one more reason beginners should not add Nandrolone to their first cycle.
Injection Site Issues: PIP, Swelling, and When to Worry
PIP, post-injection pain, is nearly universal to some degree in anyone who injects oil-based compounds. It is the local inflammatory response to the oil depot, carrier solvents, and hormone crystals depositing in muscle tissue. It varies enormously by compound (shorter-chain esters and higher-concentration formulations produce more PIP), carrier oil (MCT, grape seed, and cottonseed oils have different PIP profiles), injection site, and individual inflammatory sensitivity.
A typical PIP response: mild to moderate soreness in the injected muscle beginning 12–24 hours after injection, peaking at 24–48 hours, and resolving over the following 3–5 days. Warmth and mild swelling at the injection site are normal. This is expected and benign.
Distinguishing normal PIP from a problem requiring attention is important. A bacterial infection (abscess) at an injection site presents differently from PIP. Signs that warrant medical evaluation: escalating (rather than resolving) pain after 48–72 hours, hard lump or fluctuant swelling (rather than diffuse soreness), spreading redness beyond the injection site, fever, chills, or streaking red lines extending from the site. A sterile abscess can occur even with proper technique from crystallisation of the compound; a septic abscess requires urgent medical management with antibiotics and potentially surgical drainage. When in doubt, seek evaluation, untreated deep tissue infections can become life-threatening.
To minimise PIP: warm the oil in your hand or under running warm water for a few minutes before injection (reduces viscosity), inject slowly (30+ seconds for 1 mL), rotate sites systematically (at minimum rotate between two sites per muscle group, preferably more), and ensure sterile injection technique, new needle for every injection, swab the vial top and injection site with alcohol, do not touch anything with the needle tip after uncapping.
Selected references for major clinical, mechanistic, or protocol claims. Community-practice points may not be cited individually.