Estrogen Management for Beginners
How testosterone aromatizes to estradiol, why both high and low estrogen cause problems, when and how to use an AI, and the single most common beginner mistake in estrogen management.
- Explain the aromatization pathway from testosterone to estradiol
- Identify the distinct symptom profiles of high and low estrogen
- Know when an AI is necessary versus when to let estrogen self-regulate
- Distinguish between Arimidex and Aromasin in mechanism and dosing
- Understand estrogen management through bloodwork rather than symptoms alone
The Aromatization Pathway
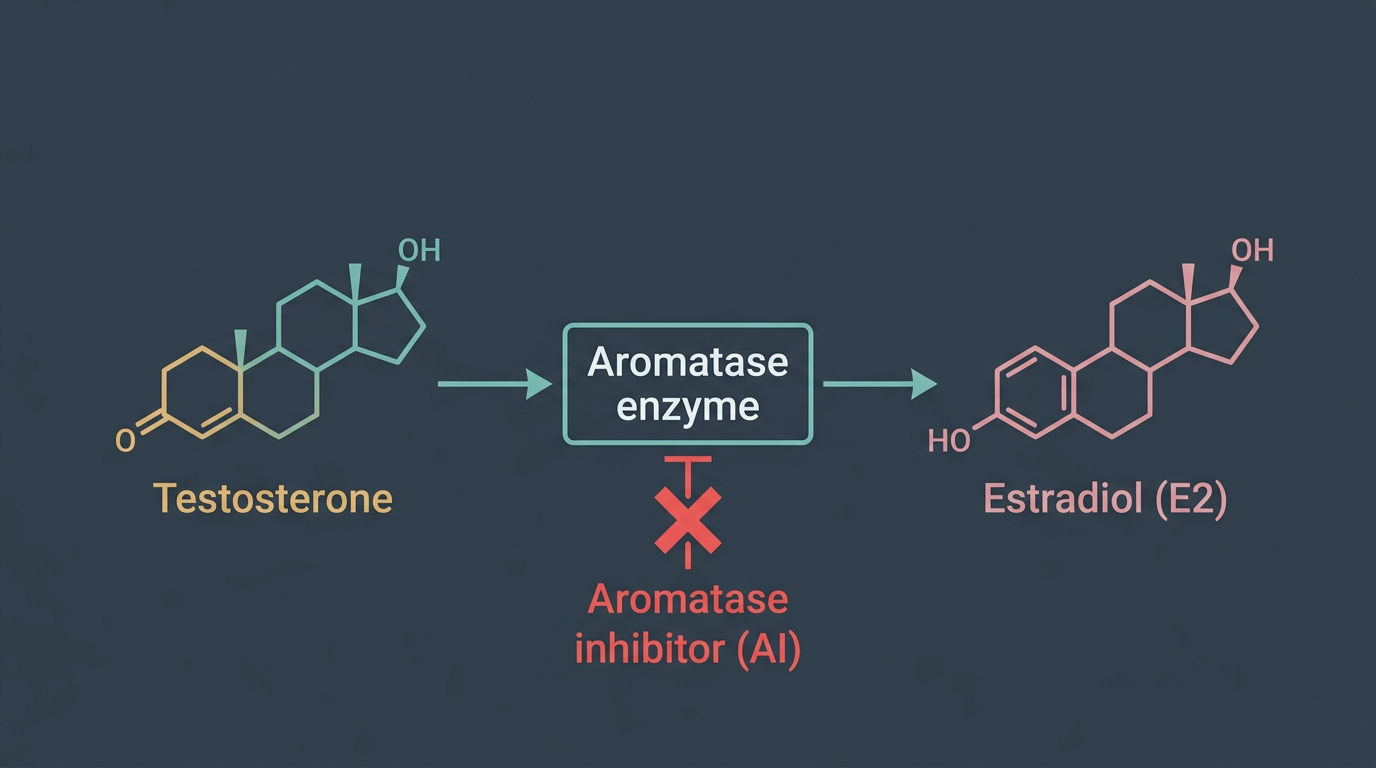
When exogenous Testosterone enters the body, it follows the same metabolic pathways as endogenous production, and one of those pathways is aromatization. Aromatase is an enzyme found in significant concentrations in adipose (fat) tissue, the liver, brain, and gonads. It converts androgens, primarily testosterone, but also Dianabol, Nandrolone (to a lesser degree), and others, into estrogens. The primary product of testosterone aromatization is estradiol, the most potent and biologically active oestrogen in the human body.
Every man produces some estradiol from his endogenous testosterone, and in physiological amounts, it is essential. Estradiol plays critical roles in bone density maintenance, cardiovascular health, libido, mood regulation, cognitive function, and joint health in men. The problem that emerges on a testosterone cycle is not that aromatization occurs, it is that when testosterone levels are 3–7× above natural, aromatization output scales upward accordingly, and estradiol can reach levels that produce symptoms.
The rate at which any individual aromatizes is highly variable and not fully predictable in advance. Body fat percentage is the strongest predictor, aromatase lives in fat tissue, so higher body fat means higher aromatization rate at any given testosterone level. Genetics, age, and individual enzyme expression also matter. Two men running identical 400 mg/week Testosterone protocols may end up with estradiol levels of 45 pg/mL and 85 pg/mL respectively, and both responses are within the range of observed variation. Bloodwork is therefore essential. Symptoms are a useful secondary signal, but numbers are the primary decision-making tool.
High Estrogen Symptoms
Elevated estradiol produces a recognisable symptom cluster, though individual sensitivity varies considerably. The classic and most feared symptom is gynecomastia, the development of glandular breast tissue under the nipple. In its early stages, this presents as nipple sensitivity or tenderness (often described as an itching, burning, or soreness around the areola), sometimes accompanied by a palpable small lump or thickening of tissue directly behind the nipple. If caught early and estradiol is controlled, this stage is typically reversible. If ignored and allowed to progress to established glandular tissue, it becomes increasingly difficult to resolve without surgical intervention.
Beyond gynecomastia, high estradiol typically produces noticeable water retention, the soft, bloated appearance that many beginners associate with their early cycle weeks. This is oestrogen-mediated water and sodium retention, not fat gain, but it obscures body composition improvements and makes the physique look less defined. Estradiol levels above 60–70 pg/mL often produce measurable physical bloating and can cause elevated blood pressure through fluid volume expansion.
Mood effects at supraphysiological estradiol are common and frequently underreported. Emotional volatility, heightened anxiety, and a general sense of instability are associated with elevated oestrogen in males, sometimes described as a “wet” emotional state compared to the assertiveness many users associate with higher androgens. Libido in the early stages of elevated estradiol may actually increase (oestrogen potentiates sexual function to a point), but at very high levels it often begins to impair erection quality and drive.
Low Estrogen: The More Dangerous Mistake
If elevated estradiol is the symptom that most beginners worry about, crashed or suppressed estradiol is the condition that most commonly results from trying to address it. Understanding why low estradiol is a significant problem, arguably worse in practice than mildly elevated oestrogen, is essential before touching an AI.
When estradiol is excessively suppressed (typically below 15–20 pg/mL), the consequences affect multiple systems. Joint pain is one of the most immediately noticeable, oestrogen plays a role in maintaining synovial fluid and joint lubrication, and crashed estradiol produces a characteristic dry, achy quality in knees, elbows, and shoulders that makes training painful and impairs performance far more than the original water retention did. Libido typically collapses entirely at very low estradiol, and erectile function can fail completely even with abundant circulating testosterone, because testosterone requires some estradiol conversion to fully exert its effects on sexual function in the brain and periphery.
Mood at crashed estradiol is often described as flat, emotionally blunted, depressed, and unmotivated, quite different from the emotional volatility of high oestrogen, but equally unpleasant. Cognitive function can feel impaired. Fatigue sets in. Skin becomes dry. These symptoms are distinctly different from high estradiol symptoms, but the beginner mistake is to treat every uncomfortable symptom as a sign of high oestrogen rather than correctly identifying the profile.
Perhaps most seriously, chronically suppressed estradiol impairs lipid metabolism in ways that mirror post-menopausal women, HDL drops, LDL rises, and the cardiovascular protective effect of oestrogen is removed. Since testosterone cycles already stress lipids, adding crashed estradiol creates a compounding cardiovascular risk load.
The key insight: mildly elevated estradiol with no symptoms is not a problem that requires treatment. Many experienced users run estradiol levels of 40–60 pg/mL on cycle with no gynecomastia issues, good libido, and good training performance. The goal of estradiol management is maintaining levels within a range that is functional and symptom-free.
When to Introduce an AI vs. Letting Estrogen Self-Regulate
Not every testosterone cycle requires an AI from day one, or at all. A common beginner error is beginning AI prophylactically, taking Arimidex or Aromasin on a fixed schedule starting week one regardless of whether estradiol is actually elevated. This approach consistently produces crashed estradiol in users who are light aromatizers, because the combined effect of the exogenous testosterone dose plus the AI drives oestrogen below physiological range.
The more evidence-based approach, particularly for lower doses (300–400 mg/week), is to start the cycle without an AI, monitor symptoms and bloodwork, and introduce an AI only if estradiol climbs into symptomatic territory confirmed by bloodwork. Have the AI on hand from day one, do order it before you need it, but hold it until bloodwork or symptoms give you a reason.
Indicators that an AI may be warranted include: nipple sensitivity or tenderness appearing on cycle; estradiol bloodwork above 50–60 pg/mL with symptoms; significant water retention affecting blood pressure or comfort. The decision to start an AI should ideally be informed by a blood test rather than symptoms alone, because the symptom profiles of high and low estradiol can overlap in some individuals and because starting an AI based on symptoms can lead to overtreatment.
At higher doses (500+ mg/week), or in users who know from prior experience that they are high aromatizers, prophylactic AI use at a low dose from the point of saturation (week 4–5) is more defensible. The key is using the lowest effective dose, the dose that holds estradiol in a functional range, confirmed with bloodwork at mid-cycle.
Arimidex vs. Aromasin: Mechanism and Dosing
The two primary AI choices for testosterone cycle management are Arimidex (anastrozole) and Aromasin (exemestane). They work through fundamentally different mechanisms, and this matters practically.
Arimidex is a competitive, non-steroidal AI. It occupies the aromatase enzyme binding site and blocks testosterone from being converted to estradiol, but does not permanently inactivate the enzyme. If you stop taking Arimidex, aromatase activity rebounds relatively quickly, and with exogenous testosterone still circulating at high levels, estradiol can rebound sharply above where it was before, sometimes producing a worse symptom spike than the original elevation. Arimidex is highly potent at suppressing estradiol, doses as low as 0.25 mg twice weekly can produce substantial estradiol reduction at 500 mg/week testosterone in moderate aromatizers.
Aromasin is a steroidal, irreversible (suicide) AI. It binds to the aromatase enzyme and permanently inactivates it, the enzyme cannot resume function after binding. New enzyme must be synthesised before aromatase activity returns. This means there is no rebound effect when you stop Aromasin, it simply stops reducing newly synthesised enzyme, and activity normalises gradually. Aromasin also has a modest anabolic property due to its steroidal structure and may have a slightly more favourable lipid profile compared to Arimidex. Typical dosing is 12.5 mg twice weekly to 25 mg every other day, with most beginners finding 12.5 mg twice weekly a reasonable starting point.
For beginners, either compound is appropriate. Arimidex is more widely available and has a well-characterised dose-response relationship that makes titration straightforward. Aromasin is preferred by many experienced users specifically because of its irreversibility (no rebound) and its steroidal character. The most important principles apply equally to both: start low, dose based on bloodwork, and never chase complete estradiol elimination.
Letrozole is the third pharmaceutical AI available, and it is markedly more potent than either Arimidex or Aromasin. A single 2.5 mg dose of Letrozole can crash estradiol to undetectable levels within 48 hours. For this reason, it has no place in routine cycle estradiol management for beginners. It is occasionally used to rapidly address an acute gynecomastia flare, but requires careful dosing and experienced judgment. Beginners should not use Letrozole as their primary AI.
The Beginner Mistake: Chasing Dry Results with an AI
There is a pervasive idea in beginner communities that estradiol suppression produces a harder, drier physique and that more AI equals better visual results. This idea is wrong, and acting on it consistently produces outcomes worse than doing nothing.
The water retention on a testosterone cycle is driven primarily by estradiol. The logic follows that if you suppress estradiol completely, the water retention goes away and you look harder. In practice, at doses below 2.5 mg Arimidex or 25 mg Aromasin per day, the relationship between AI dose and water retention is not reliable. Very aggressive AI dosing does reduce water retention, but it also produces crashed estradiol with all the associated joint pain, libido loss, and mood impairment described above. The physique “improvement” comes at a substantial quality-of-life and health cost.
The correct approach: accept that a testosterone cycle, particularly in its first half at saturation, will produce some water retention. Manage estradiol to a range that is symptom-free and healthy (roughly 20–40 pg/mL on cycle), and accept that you will look somewhat smoother than your peak leanness during active cycle phases. The lean, dry physique exists, it just comes from a well-structured diet and training approach, not from hammering an AI.
Monitoring Through Bloodwork: What Numbers to Target
Bloodwork is the only objective basis for AI management decisions. Symptoms are useful but not sufficient on their own. Target ranges for estradiol on a testosterone cycle are generally:
Below 20 pg/mL is too low. If on an AI, reduce or hold dose. Associated with joint pain, libido suppression, and mood depression. The range of 20–40 pg/mL is optimal for most men on cycle, functional libido, minimal water retention, no gynecomastia risk, preserved joint health and mood. A level of 40–60 pg/mL is elevated but manageable for many men, particularly those who are oestrogen-tolerant, watch for symptoms and consider low-dose AI if symptomatic. Above 60 pg/mL is the symptomatic range for most men, and AI intervention is appropriate if confirmed with bloodwork and symptomatic.
Draw bloodwork for estradiol management at week 4–6 of the cycle, ideally just before a scheduled injection (trough level). A sensitive assay (LC-MS/MS or equivalent) is required for accurate male estradiol measurement, the standard immunoassay used in general lab panels is calibrated for female ranges and gives unreliable results at male levels.
Selected references for major clinical, mechanistic, or protocol claims. Community-practice points may not be cited individually.