When to Stop: Red Flags and Off-Ramp Scenarios
Clear decision frameworks for identifying bloodwork red lines, cardiovascular and psychological warning signs, how to stop mid-cycle safely, and the long-term perspective on compounding cycle risks.
- Identify specific bloodwork thresholds that constitute red lines requiring action
- Recognise cardiovascular warning signs that require immediate cessation and medical care
- Monitor for psychological red flags including body dysmorphia escalation
- Know how to stop a cycle mid-run safely depending on the ester used
- Understand the long-term risk accumulation of consecutive cycles
Knowing When to Stop Is as Important as Knowing How to Start
A large fraction of harm-reduction education in the anabolic compound space focuses on how to structure cycles and manage side effects. Comparatively little emphasises the decision logic for stopping, identifying the signals that mean the correct answer is to end the cycle now, address the issue, and resume from a safer baseline if and when it is appropriate to do so.
This lesson is not about alarmism. The overwhelming majority of well-planned, monitored beginner testosterone cycles with competent bloodwork management do not produce the situations described here. But the minority that do produce these situations are more likely when preparation was insufficient, monitoring was skipped, or early warning signs were ignored. The goal is to give you a clear, pre-defined framework so that if these signals appear, you are not making the decision under stress and with incomplete information.
Bloodwork Red Lines
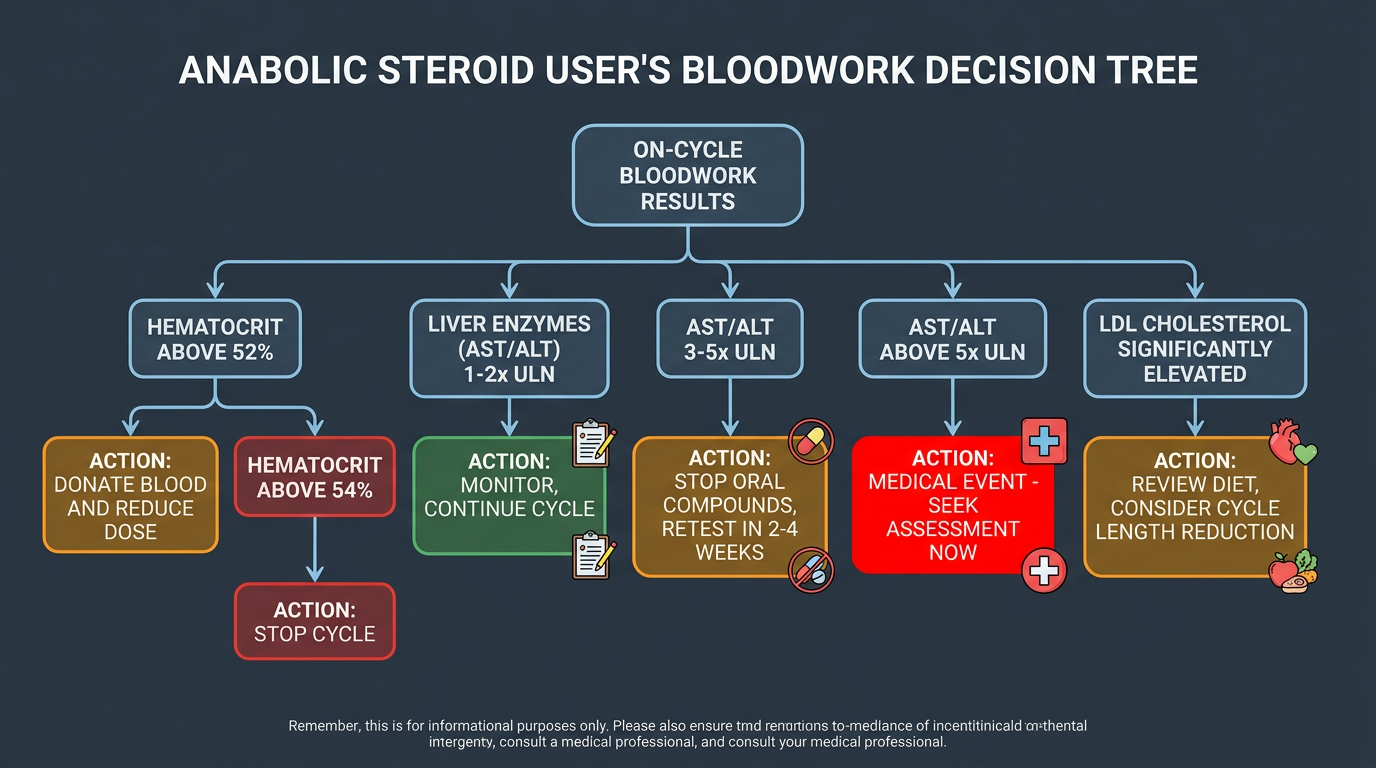
Bloodwork-derived thresholds provide the most objective criteria for cycle termination decisions. These are not bright lines that, once crossed, automatically mandate stopping, context always matters, but they are levels at which the risk-benefit equation shifts meaningfully, and action (which may or may not mean stopping) is required.
Hematocrit above 54–55%: At this level, blood viscosity is substantially elevated and thrombotic risk is meaningfully increased. The first intervention is therapeutic phlebotomy (blood donation or physician-ordered phlebotomy). If hematocrit does not decline meaningfully after phlebotomy and dose reduction, the cycle should be ended. If hematocrit is above 57–58%, cycle cessation should be considered immediately, not just as an option. Thrombotic events (pulmonary embolism, deep vein thrombosis, stroke) associated with polycythemia are catastrophic and can be fatal.
HDL below 25 mg/dL or LDL above 200 mg/dL: These represent severe lipid disruption that constitutes a real, near-term cardiovascular risk factor beyond the generally unfavourable lipid profile most cycles produce. Compounds causing this level of disruption, typically oral 17-alpha-alkylated androgens (Dianabol, Anadrol, Winstrol), should be stopped immediately. The injectable base may be continued with careful monitoring, but the oral compound should come out. Normalisation of lipids generally occurs within 4–8 weeks of cessation.
ALT or AST above 3× ULN on orals: As noted in the bloodwork lesson, 1–2× ULN elevation on oral hepatotoxic compounds is common and monitored rather than immediately treated. Above 3× ULN, the oral compound should be ceased and retested in 2–4 weeks. Above 5× ULN, this is a medical event, seek assessment. Any elevation accompanied by jaundice, right upper quadrant pain, or markedly elevated bilirubin is a medical emergency.
Estradiol persistently above 80–90 pg/mL despite AI use: This typically indicates an AI dosing problem, a compound interaction issue, or, in rare cases, an individual response requiring unusually high AI doses. Very high estradiol with persistent gynecomastia symptoms despite managed AI use may require the addition of a SERM like Tamoxifen at 20 mg/day to protect breast tissue, and possibly a dose reduction of the testosterone.
Cardiovascular Warning Signs: When to Act Now, Not Tomorrow
Certain symptoms should be treated as acute emergencies rather than cycle side effects to monitor. These are not subtle, if you experience them, the correct response is to seek immediate medical evaluation, not to post on a forum or try to manage at home.
Chest pain or pressure, especially at rest: Any new chest pain or pressure during an active anabolic cycle must be evaluated immediately. The cardiovascular risk factors associated with high-dose androgen use, elevated hematocrit, dyslipidemia, elevated blood pressure, potential left ventricular changes, place users at elevated risk for cardiac events compared to the age-matched general population. Chest pain is not a side effect to wait out.
Shortness of breath at rest or with minimal exertion: Could indicate pulmonary embolism (blood clot in the lungs), particularly in the context of elevated hematocrit and high androgen use. PE is a medical emergency with high short-term mortality if untreated.
Sudden severe headache or visual changes: Could indicate hypertensive emergency or neurological event. Blood pressure above 160/100 combined with severe headache, vision changes, confusion, or facial drooping is a stroke presentation until proven otherwise.
Leg pain, swelling, or redness (one-sided): Classic DVT (deep vein thrombosis) presentation. In the context of elevated hematocrit, this is a thrombotic event until ruled out.
For any of these presentations: stop the cycle immediately if it is safe and practical to do so, go to emergency medical care, and disclose compound use to the treating clinician. Treatment decisions may depend on knowing what compounds are active. Disclosing is in your direct medical interest regardless of legal considerations.
Persistently elevated blood pressure: Blood pressure above 140/90 consistently across multiple readings throughout the cycle is the threshold at which lifestyle intervention alone is usually insufficient and the cycle design should be reconsidered. Blood pressure above 160/100 persistently is a threshold at which cycle continuation is difficult to justify without medical oversight.
Psychological Warning Signs: Dysmorphia and Mood Dysregulation
Psychological red flags are harder to self-diagnose than bloodwork abnormalities, but they are equally real in their potential for harm. The challenge is that hormonal effects on mood and self-perception can be subtle and gradual, the shift happens slowly enough that it can be difficult to recognise from inside the experience.
Body dysmorphia escalation: If you find yourself increasingly distressed about your body despite objective improvements, spending excessive time inspecting your physique, compulsively comparing yourself to unrealistic reference points, or finding that each cycle result produces only a brief period of satisfaction before new inadequacy sets in, these are signals of escalating dysmorphic cognition. Anabolic compounds do not create this pattern, but they interact with it in a cycle-reinforcing way. The compounds produce results; the results produce temporary relief from dysmorphic distress; the relief fades; the solution appears to be more compounds or higher doses. Recognising this pattern, ideally with the help of someone who knows you well or a therapist, is important before it progresses.
Extreme mood dysregulation: Rage episodes disproportionate to triggers, pronounced emotional volatility that is affecting relationships, significant depression or anhedonia that is not responding to estradiol management. These warrant a pause. Androgenic compounds modulate multiple neurotransmitter systems (dopamine, serotonin, GABA) and the effects are not always predictable. If mood changes are severe enough to impair your relationships, work, or safety, the hormonal state you are in is not worth preserving for physique outcomes.
Psychological dependence signals: Finding that you cannot tolerate the post-cycle recovery period physically or psychologically, immediately planning the next cycle before the current one ends, or feeling that natural testosterone levels are intolerable, these are markers of psychological dependence that are worth examining seriously before the next cycle begins.
How to Stop Mid-Cycle: Ester-Dependent Approach
Stopping a cycle mid-run is not as simple as stopping any other medication, because the ester depot continues releasing compound into circulation for days to weeks after the last injection. The approach to stopping depends on which ester you are using.
Long-ester testosterone (Enanthate, Cypionate): You cannot simply stop cold and have compound clear in 24 hours. After your last injection, blood levels decline over 2–3 weeks as the ester clears. This is important for PCT timing (begin PCT 14–18 days after the last injection) but also means that if a serious adverse event occurs, you cannot immediately eliminate the compound from your system. This is one reason experienced users sometimes prefer short-ester formulations for high-risk compounds like Trenbolone, clearance is days rather than weeks if you need to stop quickly.
Short-ester testosterone (Propionate): Clears meaningfully in 4–7 days after the last injection. Begin PCT 5–7 days after last injection if stopping mid-cycle.
Oral compounds: Stop immediately. Most orals clear within 24–72 hours of the last dose, and their contribution to active compound levels is eliminated quickly.
If you are stopping a long-ester cycle mid-run due to a medical concern, do not start PCT immediately, PCT initiated while significant long-ester testosterone is still circulating will be ineffective as described in the PCT lesson. Wait for appropriate clearance based on the ester. In the meantime, manage whatever prompted the stop (blood pressure, hematocrit, etc.) with appropriate interventions.
Long-Term Perspective: The Compounding Risk of Consecutive Cycles
A first testosterone cycle, planned carefully and monitored properly, carries a manageable and largely reversible risk profile for most healthy men above 25 who have done their due diligence. The same is true for a second cycle, and generally for a third. The risk profile changes, however, with cumulative use, both because of the accumulating physiological insults of repeat cycles and because of the behavioural and psychological dynamics of escalation.
Cardiovascular remodelling is the most serious long-term concern. Repeated periods of supraphysiological androgen exposure produce left ventricular hypertrophy (increase in heart muscle mass) and changes in diastolic function that accumulate over cycles. Unlike cycle-to-cycle hematocrit or lipid changes, which largely normalise between cycles, structural cardiac changes are not fully reversible between cycles and may persist and worsen over years of use. Long-term imaging studies comparing steroid users to non-users show meaningful differences in cardiac structure and function, not uniformly severe, but consistently present in multi-year users. This is the most important long-term risk signal in this space.
The practical implication is not that doing a second or third cycle is categorically unwise. It is that each cycle should be evaluated on its own risk-benefit terms, with attention to cumulative exposure, not just the immediate risk of the individual protocol. A 10-week testosterone-only cycle at 400 mg/week once a year, with full recovery and bloodwork verification between cycles, has a very different long-term trajectory than back-to-back 20-week heavy cycles. The cycle interval, duration, compounds used, and whether full physiological recovery is achieved between cycles all matter for the long-term risk calculation.
The best habit to build from the first cycle is treating each run as a discrete, bounded event with a defined endpoint, full recovery, and a genuine gap before the next one, not a permanent state that occasionally dips to lower doses. Full HPTA recovery confirmed by bloodwork, a period of natural training to assess what was truly retained, and honest evaluation of whether the next cycle is being driven by genuine goals or by the cycle-dependence dynamic described above, these are the habits that distinguish long-term intelligent use from long-term harm accumulation.
Selected references for major clinical, mechanistic, or protocol claims. Community-practice points may not be cited individually.