Interpreting Client-Reported Side Effects
How to triage client-reported side effects, distinguish high-estrogen from low-estrogen presentations, recognise androgenic sides, identify when a side effect requires immediate medical referral, and discuss sides without playing doctor.
- Categorise the most common client-reported side effects by their likely underlying mechanism
- Distinguish the clinical picture of elevated estradiol from suppressed estradiol in how clients describe their experience
- Recognise androgenic side effects including acne severity, hairline changes, and mood effects
- Identify which side effects require immediate medical referral versus monitoring and adjustment
- Apply a communication framework for discussing side effects that educates without prescribing
Side Effects as Information
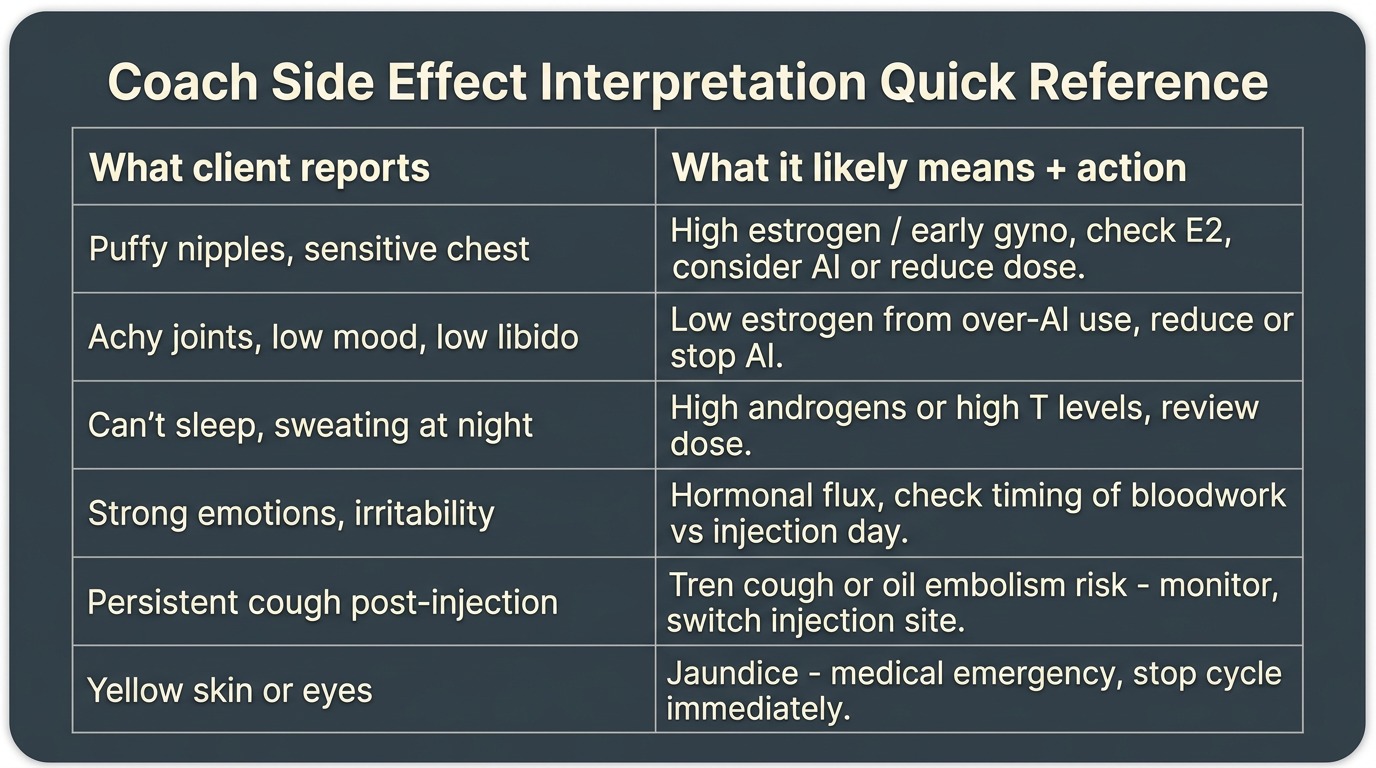
When a client reports a side effect, they are giving you information, about their hormonal environment, their individual response to a compound, and sometimes about whether their current approach is creating more risk than value. Your job is not to fix the side effect. It is to help the client understand what might be causing it, provide accurate educational context about whether it warrants concern, and determine whether the situation requires a physician’s assessment.
This distinction, between providing educational context and managing a clinical problem, is the same boundary discussed in earlier lessons, applied now to a more acute and emotionally charged situation. A client who is experiencing uncomfortable symptoms is often anxious and looking for immediate answers and interventions. The temptation to give those answers is real, but acting on it is precisely when coaches most often cross from education into medical advice.
A useful framework for side effect conversations is: describe, educate, refer. Describe what the client is reporting in detail (which requires good questioning skills). Educate about what is typically associated with those symptoms in the harm-reduction literature, compound mechanisms, known side effect profiles, what factors increase or decrease risk. Then, where appropriate, refer: tell the client what kind of medical evaluation would provide definitive answers and set up that referral.
The Common Side Effect Categories
Side effects in the context of anabolic compound use cluster into several distinct mechanistic categories. Understanding these categories allows you to triage a client’s reports more effectively.
Estrogen-related sides arise from aromatization of androgenic compounds to estradiol. They are the most common category in testosterone-based cycles and are bidirectional, both elevated and suppressed estradiol produce problematic presentations. The specific picture depends on direction.
Androgenic sides relate to DHT (dihydrotestosterone) and other compounds with high androgenic activity that interact with androgen receptors in DHT-sensitive tissues. Acne, hairline changes, and certain mood effects fall primarily into this category.
Prolactin-related sides are specific to 19-nor compounds, Nandrolone and Trenbolone in particular, that interact with progesterone receptors and can cause prolactin elevation in susceptible individuals. The side effects here overlap with high-estradiol symptoms but have a distinct profile.
Haematological and cardiovascular sides include hematocrit elevation, blood pressure changes, and the cardiac remodelling that accumulates with sustained supraphysiological androgen exposure.
Neurological and psychiatric sides are most prominently associated with Trenbolone but are documented with high-dose androgens generally: sleep disruption (including vivid and disturbing dreams), night sweats, anxiety, aggression, and mood dysregulation.
Injection-site and mechanical sides include PIP, injection-site infection, and scar tissue accumulation from repeated pinning in the same location.
High Estrogen vs. Low Estrogen: How Clients Describe Them Differently
One of the most practically useful pattern-recognition skills in PED coaching is distinguishing elevated estradiol presentations from suppressed estradiol presentations. Both are common, both cause subjective distress, and clients and coaches alike frequently misidentify one as the other, with the result that an AI dose is raised when it should be lowered, worsening the underlying problem.
The Elevated Estradiol Picture
Clients with elevated estradiol, typically above 60–70 pg/mL on a testosterone cycle, commonly describe a constellation that includes: noticeable water retention (“puffy” appearance, tight-feeling skin, increased weight that feels inconsistent with diet); mood instability characterised by emotional volatility or feeling “out of sorts” in a way that feels hormonal; reduced libido; nipple sensitivity or sensitivity behind the nipple (an early-stage indicator of gynecomastia that requires prompt attention); and sometimes a general sense of fatigue or mental fog.
The nipple sensitivity item deserves specific attention. A client who reports any breast tissue tenderness, itching, or palpable nodule behind the nipple is reporting an early-stage gynecomastia signal, the beginning of oestrogen-driven proliferation of glandular breast tissue. This is a time-sensitive situation. Gyno in its early stages (the “puffy nipple” or tender nipple phase) is typically reversible with appropriate estradiol management and, if needed, Tamoxifen use. Established, fibrosed gynecomastia is not reversible without surgery. The urgency here is real: do not wait several weeks to see if it resolves. Refer the client to a physician promptly.
The Suppressed Estradiol Picture
Clients with suppressed estradiol, most often caused by overly aggressive AI use with Arimidex or Aromasin, though occasionally seen without AI use in clients with naturally low aromatase activity, present with a different and often initially confusing picture. They frequently describe: significant joint pain, particularly in connective tissue-heavy areas (shoulders, knees, elbows), which is often attributed to the compound itself rather than estradiol crash; severe libido loss that is qualitatively different from the estrogen-excess libido suppression, it often has a more complete, flat quality; mood depression with a distinct low-energy, low-motivation, anhedonic quality; and sometimes subjective strength decreases despite continued training and nutrition.
The joint pain from low estradiol is mechanistically distinct from typical muscle soreness or PIP. Estradiol plays an important protective role in connective tissue health and joint lubrication. When it is suppressed to very low levels, below 10–15 pg/mL, joints feel dry, painful, and stiff in a way that is difficult to train through. Clients often describe this as “my joints feel like sandpaper.”
The communication challenge here is that clients on a Masteron or Winstrol-containing cycle, or on any cycle where they have been aggressively managing estradiol with an AI, often attribute the joint symptoms to “Winstrol drying out joints”, which is a common anecdotal narrative with some pharmacological basis, when in fact the joint pain is coming from estradiol that is now below therapeutic range. Distinguishing the two requires knowing the client’s current estradiol level, which is why bloodwork is the arbiter here, not symptom description alone.
Androgenic Side Effects
Androgenic sides are mediated primarily through DHT and its precursors activating androgen receptors in specific tissues. The key concept is that androgenic sensitivity is individual: the same compound at the same dose can produce significant acne in one person and none in another, significant hair thinning in one person and none in another. Genetic predisposition, primarily the density and sensitivity of androgen receptors in DHT-sensitive tissues, is the primary determinant.
Acne
Acne from androgen use is an androgenic effect mediated through sebaceous gland stimulation. It tends to appear on the upper back, shoulders, chest, and face, areas with high concentrations of sebaceous glands. Mild acne (scattered comedones and small inflammatory papules) is common and manageable with consistent hygiene practices and topical treatments. Severe cystic acne, deep, painful nodules or cysts, particularly on the face and back, is a different clinical picture that warrants medical evaluation and potentially systemic treatment.
As a coach, the relevant question is not what topical product to recommend but whether the acne presentation is in a range that the client can manage without medical intervention, or whether it has crossed into territory that requires a dermatologist. Severe cystic acne on a high-dose Trenbolone or Testosterone cycle that is significantly impacting quality of life is a referral-level concern, not a coaching intervention.
Hairline and Hair Loss
Androgen-induced hair loss (androgenetic alopecia) is mediated by DHT binding to androgen receptors in genetically susceptible hair follicles, causing follicular miniaturisation and accelerated shedding. The term “accelerated” is important: compounds do not cause hair loss in someone without genetic predisposition, they accelerate loss in someone who was eventually going to experience it anyway. For someone not predisposed, even high-dose cycles have minimal hair impact.
For clients who are predisposed, typically evidenced by a family history of male-pattern baldness, certain compounds carry much higher hairline risk than others. Trenbolone is among the most androgenic compounds in common use and carries significant hair risk for susceptible individuals. Masteron (DHT-derived) and Winstrol (DHT-derived) are similarly high-risk. Testosterone aromatizes to estradiol but also converts to DHT via 5AR, making it a moderate hair risk. Nandrolone, notably, does not convert to DHT via 5AR, it converts to dihydronandrolone, which is far weaker at the androgen receptor than DHT and is actually considered protective of hair follicles relative to testosterone-based cycles.
Finasteride is an 5AR inhibitor that blocks the conversion of testosterone to DHT, reducing DHT-mediated effects including hair loss. It is commonly used by hair-loss-conscious clients on testosterone cycles. The trade-off is that it does not work for DHT-derived compounds (like Masteron and Winstrol) that are already in an active form, and it can reduce the DHT-mediated strength and body composition benefits that some users value. The decision about Finasteride is the client’s, made with full understanding of the trade-offs, again, your role is to ensure they have accurate information, not to recommend it.
Mood and Aggression
Mood effects from androgenic compounds are real, documented, and variable. Mild increases in assertiveness, drive, and competitive motivation are commonly described and are often experienced positively by clients. Significant irritability, aggression, impulse control impairment, and emotional volatility represent a different category, one that affects the client’s relationships, professional life, and safety.
Trenbolone is disproportionately associated with significant mood effects, including severe irritability, aggression, and anxiety that can become disabling. These effects are sometimes called “tren rage” colloquially, though the mechanism is not fully characterised, it likely involves direct activity at neurological androgen receptors and possibly other receptor systems. A client reporting significant behavioural or mood changes on Trenbolone is reporting a signal worth taking seriously and discussing honestly: the compound may not be appropriate for them regardless of the physical results they are seeking.
Post-cycle mood depression is equally important to flag. The period immediately after stopping a cycle, when total testosterone is falling toward a suppressed nadir before the HPTA restarts, is a psychologically vulnerable period for many users. Low total testosterone produces fatigue, motivation loss, low libido, and mood depression that can be significant. Clients should be prepared for this and should have support structures in place. For clients with any history of depressive episodes, post-cycle management is particularly important to plan in advance.
Prolactin-Specific Sides
Prolactin elevation is a risk specific to 19-nor compounds, Nandrolone and Trenbolone, due to their progestogenic activity. The side effect profile of elevated prolactin includes: reduced libido; erectile dysfunction that has a distinct quality from low-testosterone dysfunction (often described as an inability to climax or reduced sensation rather than absent erection); and in severe cases, lactation (galactorrhoea) from male breast tissue.
These symptoms are sometimes attributed to estradiol by clients who are not aware of the prolactin mechanism, leading to mismanagement, raising AI dose to address what seems like an estradiol problem but is actually a prolactin problem. A mid-cycle prolactin draw is advisable for any client using Nandrolone or Trenbolone. Cabergoline is the standard intervention for elevated prolactin, but as with all interventions of this kind, the decision and management belong with a physician.
Side Effects That Require Immediate Medical Referral
The following presentations are immediate medical referrals:
Cardiovascular symptoms. Any chest pain, pressure, or tightness; significant shortness of breath with exertion or at rest; palpitations or arrhythmias; severe headache with elevated blood pressure. These are potential cardiac events. Call emergency services immediately.
Stroke or DVT/PE symptoms. Sudden weakness or numbness on one side of the body; slurred speech; visual disturbances; severe unilateral leg pain with swelling (potential DVT); pleuritic chest pain with or without shortness of breath and haemoptysis (potential pulmonary embolism). Emergency services immediately.
Jaundice or hepatic signs. Yellow discolouration of skin or eyes, dark urine, right upper quadrant abdominal pain, profound fatigue with associated symptoms. These suggest severe hepatic stress or failure, urgent medical evaluation.
Severe psychiatric deterioration. Suicidal ideation, psychotic symptoms, complete loss of impulse control. Clinical evaluation immediately; the conversation has moved outside coaching scope.
Signs of injection-site infection. As described in earlier lessons, spreading cellulitis, fluctuant abscess, fever, or systemic symptoms from an injection site are medical emergencies requiring prompt evaluation.
Discussing Sides Without Playing Doctor
The communication framework for side effect discussions follows the same structure described in the boundaries lesson: describe the phenomenon educationally, be honest about what level of concern it warrants, and be clear about what kind of professional is positioned to actually address it.
A useful phrase structure: “What you’re describing sounds consistent with [mechanism description], that’s a documented effect associated with [compound]. The harm-reduction literature generally describes that as [characterisation of severity]. My strong recommendation is that you get bloodwork done to confirm what’s actually happening before making any changes, and discuss the results with a physician before adjusting anything. In the meantime, here is what the monitoring framework says about this marker…”
This approach provides genuine value to the client. It does not leave them with “I don’t know, go see a doctor”, it gives them a framework for understanding what might be happening and what a proper assessment would involve. It does not prescribe a specific intervention. And it clearly positions the physician as the authority for clinical management while preserving your role as the person who helps the client understand the context.
Selected references for major clinical, mechanistic, or protocol claims. Community-practice points may not be cited individually.