Screening and Red-Flag Detection
How to evaluate a new client's health readiness, bloodwork prerequisites, psychological red flags, and what to do when a client does not meet the bar for responsible coaching.
- Define the health and bloodwork prerequisites a responsible coach requires before coaching anyone using compounds
- Identify psychological red flags including body dysmorphia indicators and unrealistic expectations
- Apply age and training maturity standards as non-negotiable gatekeeping criteria
- Describe a structured intake process for evaluating a new client's readiness
- Explain how to decline or redirect a client who does not meet the bar without burning the relationship
The Coach’s First Responsibility: Screening
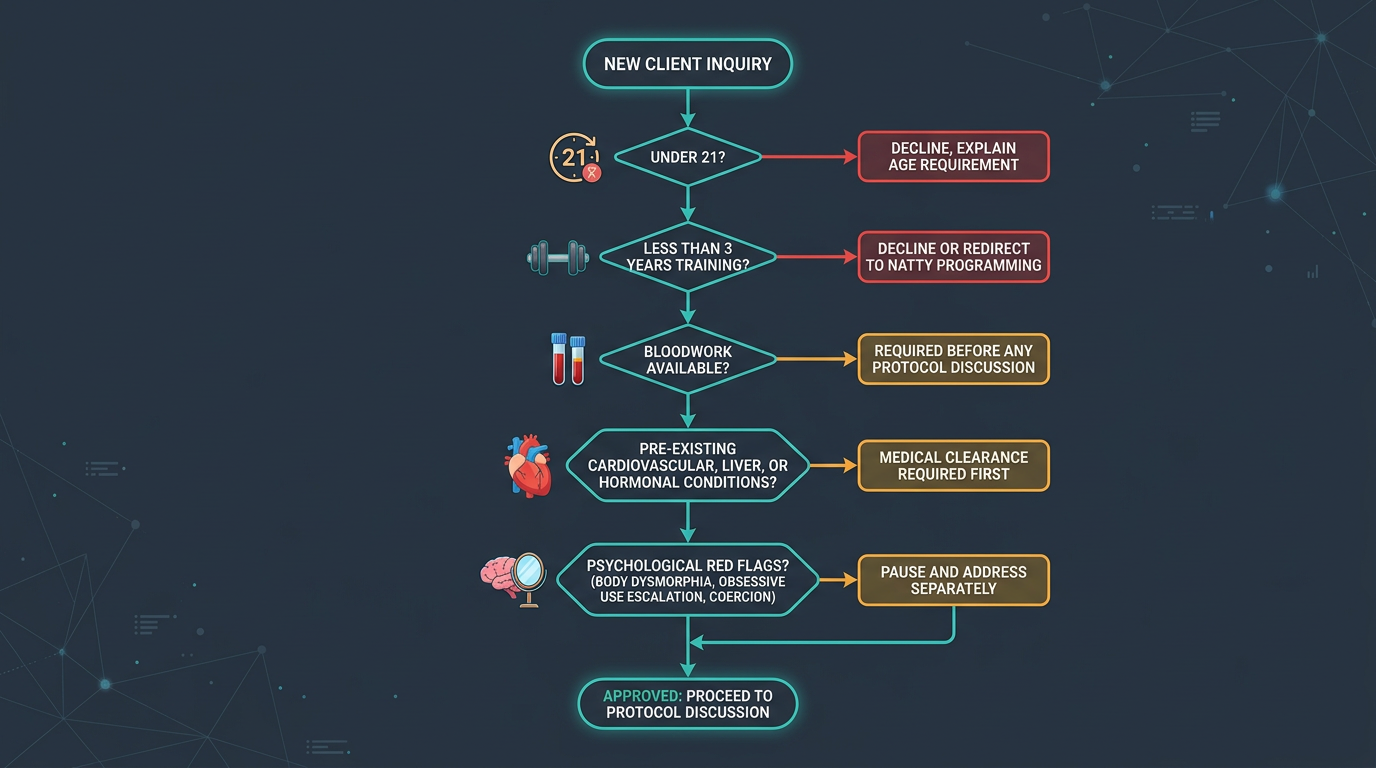
Coaching clients who use performance-enhancing compounds carries a specific set of professional obligations that begin before any programming is written, before any compound is discussed, and before a coaching relationship is formalised. The first obligation is screening, a structured, honest evaluation of whether the client in front of you is an appropriate person to coach in this context at all.
The foundation of responsible practice. A coach who accepts every client regardless of health status, psychological readiness, or training background creates liability for themselves and genuine harm for clients who were not ready. Screening protects the client, protects you, and maintains the integrity of harm-reduction-informed coaching as a practice.
CompoundLab is a tool you can use during this process, both to assess a client’s understanding of the compounds they intend to use, and to structure educational conversations about what responsible use actually requires. But the screening conversation itself is yours to lead, and no platform can substitute for a direct, structured assessment.
Health Readiness and Bloodwork Prerequisites
The single most important gating criterion before coaching any client who uses or intends to use anabolic compounds is comprehensive bloodwork. A client who does not have recent baseline bloodwork is not ready to receive coaching in this domain, full stop. This is a genuine safety requirement.
Baseline bloodwork before a first cycle establishes the client’s individual reference points across every marker that exogenous compounds will affect. Without that baseline, neither you nor the client can answer the fundamental question: what did this compound do? You cannot distinguish a compound-induced lipid disturbance from a pre-existing one. You cannot tell whether low post-cycle total testosterone represents prolonged suppression or simply where the client’s HPTA was before any intervention. Pre-cycle bloodwork is the minimum viable starting condition.
At a minimum, the baseline panel a client should present before beginning a coached PED-assisted protocol should include: complete blood count (CBC) with differential to capture baseline hematocrit and hemoglobin; comprehensive metabolic panel (CMP) covering kidney and liver function markers including ALT, AST, and GGT (liver enzymes); a full lipids panel (total cholesterol, HDL, LDL, triglycerides); a hormone panel including total testosterone, free testosterone, estradiol, LH, and FSH; SHBG; TSH for thyroid baseline; and PSA in clients over 30 or any client with a family history of prostate disease.
Beyond the panel itself, evaluate the timing and context of the results. Bloodwork drawn during or immediately after a previous cycle is not a useful baseline. It reflects an altered hormonal state rather than a natural one. Ideally you want bloodwork drawn at least 8–12 weeks after the last cycle has fully cleared, including allowing time for long-ester compounds like Nandrolone Decanoate or Testosterone Cypionate to fully wash out before the draw.
Cardiovascular readiness is equally important. Ask about resting blood pressure (values consistently above 140/90 require medical evaluation before any cycle), family history of early cardiovascular disease, personal history of cardiac events, and any diagnosed cardiovascular conditions. Exogenous androgens raise hematocrit, suppress HDL lipids, and promote vascular remodelling. A client with pre-existing cardiovascular compromise needs physician clearance before you even consider coaching them in this space.
Apply the same scrutiny to hepatic and renal function. A client with elevated baseline liver enzymes cannot run hepatotoxic oral compounds like Dianabol, Anadrol, or Winstrol, and you should not coach them toward doing so until the elevation is investigated and resolved. Elevated creatinine or reduced GFR (glomerular filtration rate) raises concerns about renal function that exogenous androgens can stress further.
Age and Training Maturity Requirements
Age is the most non-negotiable criterion in this framework, and it is one where responsible coaches hold the line consistently.
The HPTA and central endocrine system are not fully mature until the mid-twenties, typically around age 25 as a working minimum. Before that threshold, the hypothalamic-pituitary axis is in active developmental flux. Exogenous androgens impose suppression on a system that is still building its own regulatory architecture. The risk of permanent or prolonged dysfunction is substantially elevated compared to fully mature adult use, and the cost of that dysfunction, persistent low total testosterone, impaired fertility, and cascading hormonal effects, falls on a person who has decades ahead of them.
A blanket minimum age of 25 is the responsible professional standard. Some coaches apply 23 as a minimum for select compounds with a more modest risk profile (typically Anavar or low-dose Testosterone under close monitoring), but 25 is the defensible benchmark. Any client under this threshold should be declined for PED-related coaching regardless of how mature they seem, how much they claim to have researched, or how persistent they are. The pressure a young client applies is often itself a signal that they are not ready.
Training maturity is a distinct but related criterion. A client who has not been training seriously and consistently for at least two to three years is not deriving maximum benefit from their natural hormonal environment, which means the marginal gain from exogenous compounds is proportionally lower and the relative risk higher. Training maturity also signals the practical discipline required for responsible use: the commitment to consistent injection schedules, monitoring protocols, and dietary compliance that separates meaningful outcomes from reckless exposure. A client who has trained for six months and wants to jump on Trenbolone is telling you something important about their risk framework.
Weight and body composition context matters too. Clients who are significantly overweight (elevated body fat percentage) have more active aromatase in adipose tissue, meaning they aromatize at higher rates and are more prone to estradiol-related sides including gynecomastia and water retention. Advising a high-body-fat client into a high-aromatization compound like Testosterone at aggressive doses before they have addressed their body composition creates a more complex side effect management challenge for limited practical benefit. Reaching a reasonable body composition baseline first is sensible gatekeeping.
Psychological Red Flags
Health metrics and bloodwork are the objective screening layer. Equally important, and often neglected, is the psychological screening layer.
Body dysmorphia in the fitness context, sometimes called muscle dysmorphia or “bigorexia,” is a condition characterised by a persistent and distorted belief that one’s body is inadequately muscular or developed regardless of actual appearance or objective assessment. It drives compulsive training, disordered eating, and, critically, an intense motivation to use performance-enhancing compounds to close a gap that does not exist in objective terms but feels overwhelming subjectively. A client with muscle dysmorphia will have unrealistic expectations of what compounds will deliver, an inability to accept normal progress timelines, a tendency to escalate doses or add compounds prematurely when results feel insufficient, and significant distress when training is missed or results plateau.
Screening for muscle dysmorphia is a clinical responsibility, not a coaching one. But as a coach you are looking for behavioural and conversational signals: Does the client express significant distress about their current appearance that is disproportionate to what you observe? Do they describe previous compound use as having “not worked” despite objective evidence of gains? Do they reference specific physiques (often of professional bodybuilders or social media figures) as a target without acknowledging the implausibility of those comparisons? Are they dismissive of timelines or resistant to the idea of building a foundation before compounds? These patterns, individually, are worth a careful, direct conversation before proceeding.
Unrealistic expectations are a related but broader category. A client who expects Testosterone Enanthate to produce 20 pounds of muscle in 12 weeks has absorbed information from unreliable sources, and the inevitable gap between expectation and outcome creates the pressure to do more, more compound, higher dose, additional compounds stacked. Managing expectations is not just about honesty; it is a safety practice. A client who understands realistic outcome ranges is far less likely to make dangerous decisions mid-cycle.
Pressure dynamics are worth flagging explicitly. If a client is using compounds because a partner, teammate, coach, or social group is pressuring them to, rather than because they have arrived at an informed, autonomous decision, the psychological groundwork for responsible use is not present. Compound use under social pressure lacks the informed consent foundation that responsible use requires. It also creates a dynamic where the client may be unwilling to disclose side effects honestly or pause a cycle when they should, because stopping feels like a social failure.
Finally, be alert to signs of current mental health instability: recent trauma, active depressive episodes, anxiety disorders that are not managed, or a history of psychiatric conditions that androgens are known to exacerbate. High-dose androgen use carries documented psychiatric risk, aggression, mood instability, and depressive episodes during and especially after cycles. A client who is psychologically fragile at baseline faces a meaningfully higher risk of serious psychiatric events.
When a Client Doesn’t Meet the Bar
Deciding a client is not ready is not the end of the relationship, it is an opportunity to define what readiness looks like and build a pathway to it.
A responsible decline is specific, non-judgmental, and forward-looking. Rather than “I won’t coach you on this,” the framing is: “Here is what needs to be in place before I can responsibly support you in this. Let’s work on getting there.” If the barrier is incomplete bloodwork, outline exactly what panel you need and when to revisit. If the barrier is age, be direct about why the threshold exists and what to do with the time between now and maturity, build base strength, refine diet, and get genuinely informed. If the barrier is psychological, the conversation is more delicate but the principle is the same: here is what needs to change, and here is how I can support that.
Some clients will not accept this and will seek coaching elsewhere. That is their right. Your professional obligation is not to retain every client at any cost, it is to maintain standards that you can defend to yourself and, if necessary, to others. A coach who waves through every client regardless of readiness is not providing a valuable service; they are providing social permission for decisions people have already made, which is a much less meaningful and much more legally exposed role.
Document your screening process and decisions. A written intake protocol that covers the questions you asked, the information the client provided, and the rationale for your decision creates a record of professional practice that matters both for your own standards and for your protection in the event of a negative outcome.
Selected references for major clinical, mechanistic, or protocol claims. Community-practice points may not be cited individually.