TRT Candidacy and Diagnosis
A clinical introduction to testosterone replacement therapy, who qualifies, how it is diagnosed, and how it differs fundamentally from anabolic cycling.
- Understand the clinical definition of hypogonadism and how it differs from symptomatic low testosterone
- Recognize the symptom profile that leads clinicians to investigate TRT candidacy
- Understand how bloodwork is interpreted in the context of TRT diagnosis
- Distinguish TRT as a medical protocol from supraphysiological anabolic cycling
- Identify contraindications and populations who should avoid TRT
What TRT Is
Testosterone Replacement Therapy, commonly abbreviated TRT, is a medically supervised protocol in which exogenous Testosterone is administered to individuals whose endogenous testosterone production is clinically insufficient. The goal is restoration, not enhancement. This distinction is not merely semantic: it defines the intent, the dosing philosophy, the monitoring requirements, and the risk-benefit calculus of the entire protocol. TRT is not a performance-enhancement strategy, and understanding that boundary is the foundation of everything that follows in this track.
At its core, TRT addresses a condition called hypogonadism. Primary hypogonadism occurs when the testes themselves fail to produce adequate testosterone, often due to genetic conditions like Klinefelter syndrome, physical injury, infection, or chemotherapy damage. Secondary hypogonadism, also called hypogonadotropic hypogonadism, occurs when the hypothalamic-pituitary axis fails to send the right signals to the testes. In secondary hypogonadism, LH (luteinizing hormone) and FSH (follicle-stimulating hormone) are typically low or low-normal, reflecting inadequate signaling from the pituitary rather than testicular failure per se.
Symptoms That Prompt Investigation
The symptom profile of low testosterone is wide-ranging and often non-specific. Fatigue that is not explained by sleep disorders, thyroid dysfunction, anemia, or depression is one of the most commonly reported symptoms. Low libido frequently co-presents with erectile dysfunction. Cognitive fog, the subjective sense that one’s mental sharpness and working memory have degraded, is reported by many men with low testosterone.
Body composition shifts are perhaps the most visible marker: a loss of lean muscle mass despite consistent training, an increase in adiposity particularly in the abdominal and chest regions, and a general reduction in the anabolic responsiveness to resistance exercise. These changes occur because Testosterone is a key regulator of protein synthesis, satellite cell activation, and fat oxidation.
How TRT is Diagnosed
Diagnosis of hypogonadism requires at least two separate morning blood draws showing total testosterone below the laboratory reference range, typically below 300 ng/dL in the United States. Morning testing is critical because testosterone follows a circadian rhythm, with peak levels occurring in the early morning hours.
Beyond total testosterone, a complete hormonal panel should include free testosterone and bioavailable testosterone. SHBG binds testosterone in the bloodstream and renders it inactive. LH and FSH should also be measured to distinguish primary from secondary hypogonadism. A complete metabolic panel, lipids, complete blood count, thyroid function, prolactin, and estradiol round out the baseline evaluation.
TRT vs. Anabolic Cycling
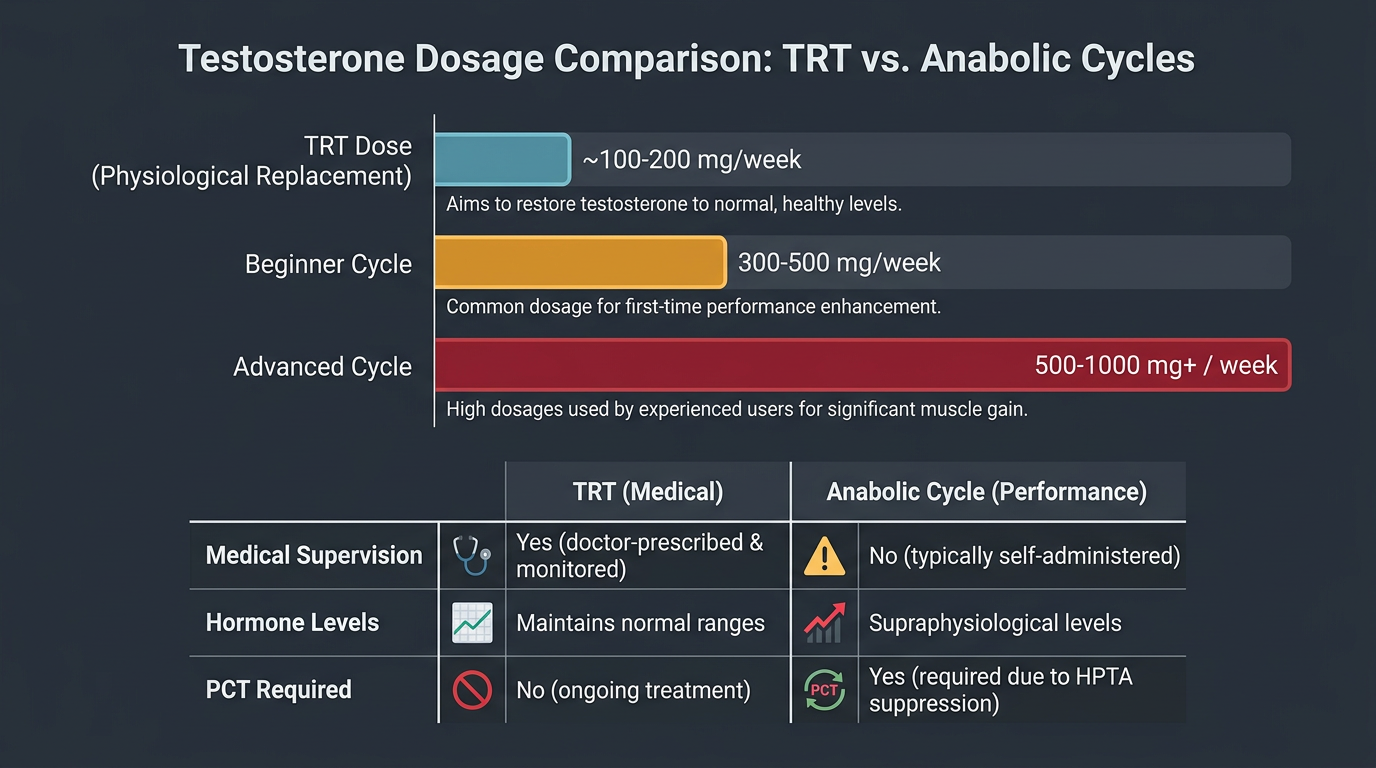
This is perhaps the most important conceptual boundary in this entire curriculum. TRT is a medical protocol that restores testosterone to the physiological range. Anabolic cycling is a practice of administering supraphysiological doses of Testosterone and/or other anabolic-androgenic compounds with the explicit goal of exceeding that physiological range to drive enhanced muscle hypertrophy, strength, or athletic performance.
A typical TRT dose of Testosterone is usually between 100 and 200 mg per week, adjusted to achieve total testosterone levels somewhere between 500 and 900 ng/dL. A typical anabolic cycle might use 400–600 mg per week as a foundation, with additional compounds added on top. The aromatization rate, the degree of suppression of the HPTA, the hematocrit elevation, the cardiovascular strain, and the potential for androgenic side effects all scale with dose in ways that make TRT and cycling genuinely different categories of risk.
Who Should Not Use TRT
Not everyone with low testosterone is an appropriate TRT candidate. A history of hormone-sensitive prostate cancer is an absolute contraindication to TRT in most clinical guidelines, because Testosterone and its conversion to DHT via the 5AR enzyme can accelerate prostate cancer progression. Polycythemia, an elevated red blood cell mass leading to dangerously high hematocrit, is either a contraindication or requires very careful management. Men who are actively trying to conceive should understand that exogenous Testosterone suppresses LH and FSH, leading to dramatically reduced sperm production.
Selected references for major clinical, mechanistic, or protocol claims. Community-practice points may not be cited individually.