Bloodwork and Monitoring on TRT
A comprehensive guide to the labs every TRT user needs, how often to test, and what the results mean for long-term health management.
- Identify the full panel of laboratory tests needed for TRT monitoring
- Understand hematocrit elevation on TRT and when blood donation becomes necessary
- Interpret lipid changes in the context of TRT and cardiovascular risk
- Understand the role of PSA monitoring in aging TRT users
- Design an appropriate monitoring schedule for both initiation and maintenance phases
Why Monitoring Is Non-Negotiable

Testosterone is a powerful anabolic and androgenic hormone with downstream effects on red blood cell production, lipids, prostate tissue, cardiovascular physiology, and liver enzymes. Initiating TRT without a structured monitoring protocol is the clinical equivalent of prescribing a chronic medication and never following up.
The Full TRT Monitoring Panel
A comprehensive TRT monitoring panel covers five domains: hormone levels, red blood cell physiology, cardiovascular markers, hepatic health, and prostate assessment.
Hormone Panel: Total testosterone and free testosterone (or SHBG to calculate it) confirm that the dose is achieving the intended level. Estradiol (sensitive assay) should always accompany testosterone monitoring. LH and FSH are typically suppressed to near-zero on exogenous Testosterone and do not need to be tested routinely once suppression is confirmed.
Red Blood Cell and Hematologic Panel: A complete blood count (CBC) is essential. Hematocrit above approximately 52–54% increases blood viscosity substantially, raising the risk of thrombotic events, deep vein thrombosis, pulmonary embolism, stroke.
Cardiovascular and Metabolic Panel: A fasting lipids panel should be monitored because Testosterone therapy consistently lowers HDL. Blood pressure should be measured at every check-in, as both the androgenic effects of Testosterone and elevated hematocrit can contribute to hypertension.
PSA Monitoring: PSA (prostate-specific antigen) should be tested in men over 40. TRT causes a modest expected increase in PSA in the initial months. A PSA increase of more than 1.4 ng/mL above baseline in any consecutive 12-month period warrants urological referral.
Hematocrit Elevation
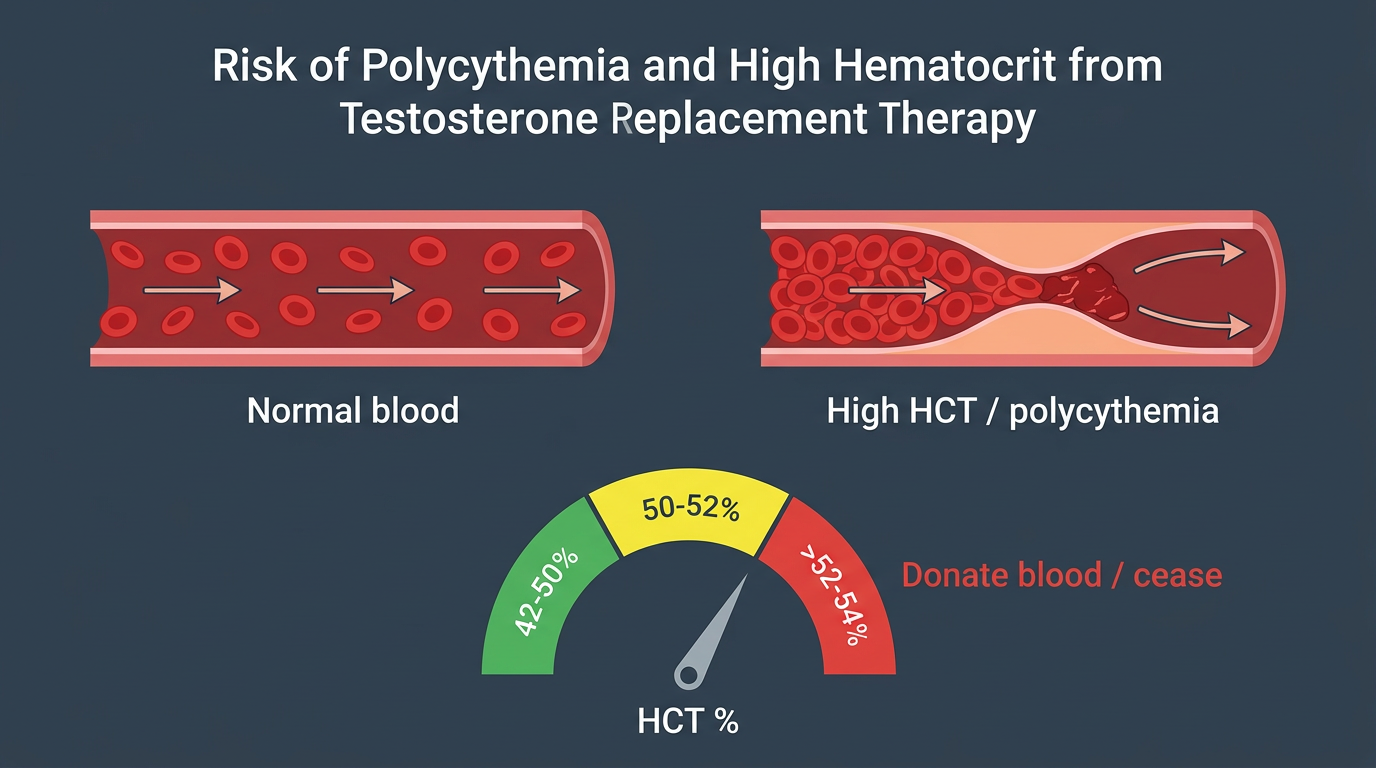
Testosterone stimulates the kidneys to produce erythropoietin (EPO), which drives increased red blood cell production. The primary management tool for elevated hematocrit is therapeutic phlebotomy, blood donation. Donating a unit of blood typically reduces hematocrit by 2–4 percentage points. If hematocrit elevation is persistent despite regular donation, options include dose reduction, switching to a shorter-ester formulation with more frequent smaller doses, or switching to a topical preparation.
Monitoring Frequency
The first 6 months are a titration and baseline-establishment phase requiring more frequent testing. Most TRT clinicians recommend an initial check at 6–8 weeks after starting, and a second check at 3–4 months. Once stable for 6 months with all parameters in acceptable ranges, most patients can transition to twice-yearly hormone levels and CBC, with annual lipids and PSA.
Selected references for major clinical, mechanistic, or protocol claims. Community-practice points may not be cited individually.