TRT, Cycling, and Blast-and-Cruise Boundaries
An honest, nuanced exploration of how TRT and anabolic cycling differ in intent, dose, and risk, and how to approach conversations with a physician about TRT honestly.
- Articulate the principled differences between TRT and anabolic cycling in purpose, dose, and risk profile
- Understand what blast-and-cruise means and how it differs from therapeutic TRT
- Recognize the pattern of supraphysiological use framed as TRT
- Assess the risk differential between TRT doses and cycle doses honestly
- Understand how to approach a physician about TRT with accuracy and integrity
Clarity About What You’re Doing
The label “TRT” has become, in parts of the fitness world, a semantic shield. It lets a person describe exogenous testosterone use in language that sounds medical, disciplined, and low-risk even when the underlying behavior is plainly performance-enhancing. That is not a harmless vocabulary issue. It affects self-honesty, physician communication, risk assessment, and the way people justify escalation.
Clarity about whether you are doing TRT or cycling is not moralizing. It is a harm-reduction prerequisite. If you mislabel enhancement as therapy, you are much more likely to underestimate risk and much less likely to build the right monitoring framework around what you are actually doing.
What Counts as TRT
Therapeutic TRT has several defining characteristics.
First, there is a real clinical context. TRT is initiated because there is a documented androgen deficiency, confirmed on repeated morning labs, paired with a meaningful symptom burden. The goal is to restore a deficient state toward normal function.
Second, the dosing intent is restorative rather than maximizing. A TRT protocol aims to produce physiological testosterone levels, not the highest level a clinic can justify on paper. The purpose is symptom relief and long-term stability, not constant upward pressure on strength, fullness, or gym performance.
Third, the compound profile is simple. Therapeutic TRT is testosterone-centered. The moment a protocol includes additional anabolic compounds like Nandrolone, Trenbolone, Masteron, or Anavar for physique or performance goals, you are no longer in an honest replacement framework, regardless of what the testosterone dose is.
Fourth, the monitoring philosophy is medical rather than opportunistic. Labs are used to confirm therapeutic range, track safety markers, and make conservative adjustments. That is very different from using labs to see how much enhancement you can get away with before a clinician objects.
The Simplest Real-World Test
If you want a simple test for whether something is TRT or a cycle, ask four questions:
- Was it started because of genuine hypogonadal symptoms and confirming labs?
- Is the goal to function normally or to perform above normal?
- Are the resulting testosterone levels physiological or clearly supraphysiological?
- Is testosterone the only anabolic drug in the plan?
If the answers drift toward performance, supraphysiology, and stack-building, then whatever the label says, the behavior is cycling.
The Dose Difference Is Real, But It Is Not the Only Difference
People often reduce the TRT-versus-cycle question to milligrams per week. Dose matters, but intent, outcomes, and stack structure matter too.
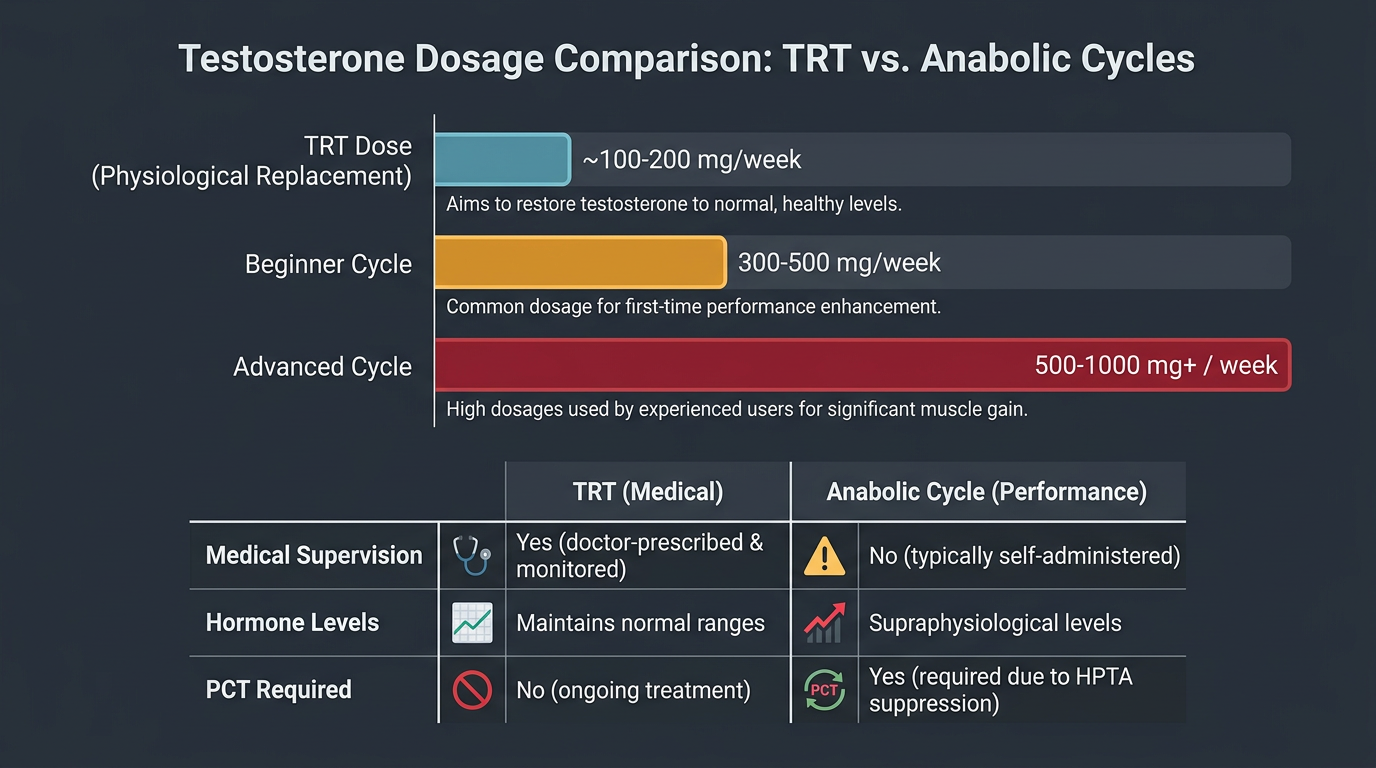
A true TRT dose is usually intended to land a man in a physiological hormonal range. A cycle dose is intended to exceed it. That distinction is not merely academic. Once testosterone levels move well above the range male physiology is designed to operate in chronically, you are no longer replacing a deficit. You are pushing an anabolic state.
But even if the testosterone number itself is not extreme, the addition of non-TRT compounds changes the entire framework. A “TRT base” with added Anavar for a cut, or with Nandrolone for joint comfort and size, is not therapeutic replacement. It is a cycle built on a testosterone foundation.
Why the Fitness World Blurs the Line
People blur this line for understandable reasons. “TRT” sounds legitimate. It sounds measured. It sounds safer than “I am using anabolic hormones for performance.” Some men also move into enhancement gradually, so the transition feels subtle: a slightly higher dose, then a little more because symptoms still seem “off,” then a short oral, then a deca add-on, then a year later the person is effectively blast-and-cruise while still describing himself as a TRT patient.
That drift matters because language shapes behavior. A man who thinks of himself as being on medical therapy is less likely to ask the right questions about cardiovascular load, fertility loss, dependence patterns, exit strategy, and cumulative exposure. He may still be monitoring, but he is often monitoring a cycle through a therapeutic mental frame.
Blast-and-Cruise Is Not TRT
Blast and cruise is a distinct long-term lifestyle choice in which a user maintains a year-round cruise dose of Testosterone and periodically increases to higher-dose blast phases. From a harm-reduction perspective, it can be safer than repeatedly going fully on and fully off very heavy cycles. But safer than one bad option does not make it the same thing as TRT.
The cruise phase in blast-and-cruise is often described as “basically TRT.” Sometimes the weekly dose overlaps numerically with TRT ranges. That is exactly why people confuse them. But context matters. In blast-and-cruise, the cruise phase is not being used to treat diagnosed hypogonadism. It is being used to remain hormonally supported between enhancement phases. The surrounding purpose changes the meaning of the cruise.
This difference also matters for fertility and long-term planning. A true TRT patient may accept suppression because symptom relief is the central medical goal. A blast-and-cruise user is accepting chronic suppression as the maintenance cost of ongoing performance enhancement. That is a different trade, and it should be named honestly.
What “TRT+” Usually Means
Many protocols marketed online as TRT are really “TRT+” arrangements. That usually means one of three things:
- Testosterone dosed high enough to produce clearly supraphysiological levels while still being described as replacement.
- Testosterone plus an oral or injectable anabolic compound.
- Testosterone plus a rotating set of ancillaries intended to support a higher-than-therapeutic hormonal environment.
Calling these protocols “TRT+” is at least more honest than pretending they are standard replacement, but it still matters to understand that the risk profile is no longer that of straightforward TRT. Once doses and compounds are chosen for physique or performance return rather than restoration of normal function, the framework has shifted.
Honest Risk Assessment: TRT Doses vs. Cycle Doses
At TRT doses that keep testosterone in a physiological range, the main monitored concerns are usually manageable: hematocrit elevation, HDL reduction, mild PSA changes, acne in some users, hair-loss acceleration in predisposed men, and fertility suppression. These are real issues, but they usually exist within a medical risk-benefit discussion.
At typical cycle doses of Testosterone such as 400-600+ mg/week, especially when combined with compounds like Trenbolone, Nandrolone, Dianabol, or Anavar, the risk profile changes qualitatively, not just quantitatively. Hematocrit often rises more sharply. HDL suppression is deeper. Blood pressure is more likely to worsen. Estrogen management becomes more difficult. Recovery becomes less predictable. Additional compounds introduce risks that simply do not belong in a therapeutic framework at all.
Trenbolone is the clearest example. Its cardiovascular, neurological, and psychiatric burden is not an extension of TRT. It is a separate performance-drug risk class. Once that kind of compound enters the picture, continuing to describe the protocol as TRT is not an innocent shorthand. It actively obscures the risk reality.
What Physicians Are Actually Working With
Physicians can only manage what they are actually told. If a patient says he is “on TRT” but is really using supraphysiological testosterone, or adding additional anabolic compounds, the clinician is working with a false model. That affects interpretation of labs, assessment of side effects, fertility counseling, and decisions about blood pressure, lipids, or hematocrit.
A doctor who thinks he is managing ordinary replacement may underestimate why the patient has severe HDL suppression, disproportionate erythrocytosis, or unusual psychological symptoms. The patient may then conclude that the physician “doesn’t understand TRT,” when the clinician was never given an accurate picture of the protocol.
How to Talk to a Doctor About TRT Honestly
Be accurate about symptoms. Be honest about prior anabolic history. Be honest about fertility goals. If you have used supraphysiological doses before, say so. If your goal is partly performance, acknowledge that rather than trying to backdoor it through therapeutic language.
This matters not because the doctor needs to approve your identity, but because the medical risks are different when a person has prior suppression history, prior anabolic exposure, or active enhancement goals. A physician working from an accurate history can manage care. A physician working from a sanitized story cannot.
The Self-Honesty Test
The clearest self-honesty question is not “what does my clinic call this?” It is: what would happen if the dose were lowered until labs, symptoms, and physiology were clearly in normal therapeutic territory and stayed there?
If that sounds like the goal, you are describing TRT.
If that sounds like losing the whole point of the protocol, you are probably describing enhancement.
There is nothing gained, from a harm-reduction perspective, by pretending those are the same thing. The safest path is to call the protocol what it is, accept the corresponding risk profile, and build your decision-making around reality rather than around a softer label.
Selected references for major clinical, mechanistic, or protocol claims. Community-practice points may not be cited individually.