Fertility, Side Effects, and Long-Term Considerations
How TRT affects fertility, which side effects to monitor proactively, and what the current evidence says about long-term health outcomes on testosterone replacement.
- Understand how exogenous testosterone suppresses the HPTA and affects spermatogenesis
- Evaluate the role of HCG in maintaining testicular function on TRT
- Recognize androgenic side effects including hair loss and their genetic basis
- Understand polycythemia as a TRT complication and how to manage it
- Assess the current state of long-term cardiovascular evidence for TRT
How TRT Affects the Hormonal Axis
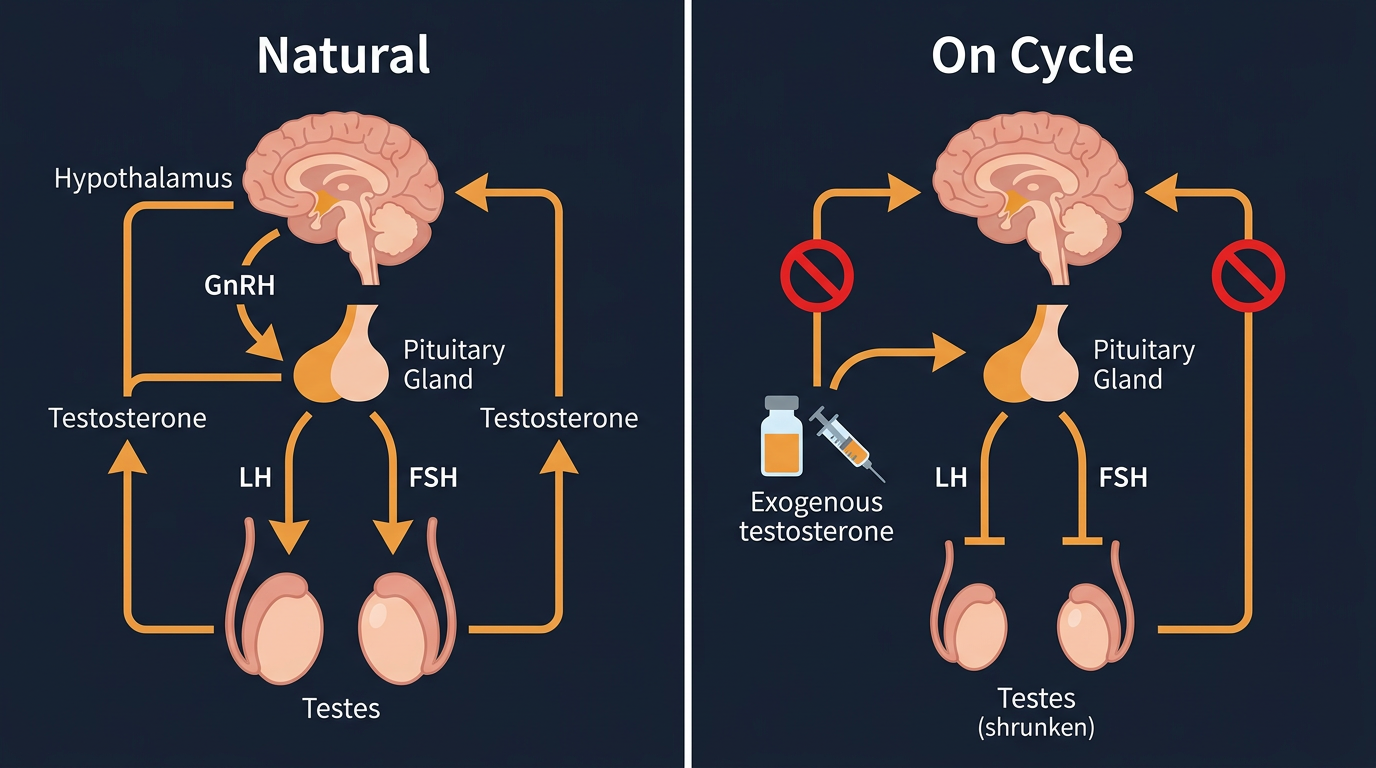
One of the most important physiological consequences of introducing exogenous Testosterone, even at true replacement doses, is suppression of the body’s own hormonal signaling system through the HPTA. The hypothalamus and pituitary detect that androgen levels are now being supplied from outside the body and reduce GnRH, LH, and FSH output. This is not a side effect in the usual sense. It is the expected physiological response to exogenous hormone.
The practical consequence is that the testes are no longer receiving the same internal stimulation they would receive in an untreated man. Endogenous testosterone production falls. Testicular volume often decreases. Sperm production usually declines, sometimes dramatically. This catches a lot of men off guard because they assume “replacement dose” means their reproductive system will continue working normally. It usually does not.
Fertility on TRT
The most important fertility concept on TRT is that fertility is not binary. Men do not all respond the same way. Some remain fertile enough to conceive while using TRT. Others see sperm count fall to very low levels or to zero. Assuming you will be the exception without checking is how people get blindsided.
Spermatogenesis depends on more than circulating testosterone. It depends on intratesticular testosterone production and coordinated LH/FSH signaling. TRT suppresses exactly the upstream signals that support that environment. A man can have normal or even high serum testosterone on paper while his fertility is meaningfully compromised. Fertility planning and symptom improvement therefore overlap, but they are not the same goal.
For a man who may want children in the near future, this issue should be addressed before starting therapy, not after six months of suppression. “I feel much better on TRT, but now we are trying to conceive” is one of the most common avoidable problems in this category.
Fertility Is a Timing Question, Not Just a Biology Question
The right fertility conversation depends heavily on timeline.
If a man wants children soon, TRT may be the wrong first move or may need a fertility-preserving strategy from day one. If children are a distant possibility rather than an immediate goal, he still needs to understand that time on TRT is often time spent under ongoing gonadotropin suppression. If he already has children and is certain he does not want more, the fertility tradeoff may matter less, but it still should be understood explicitly rather than discovered by accident.
There is also a difference between “maintaining some testicular function” and “guaranteeing fertility.” Those are not the same thing. Many online conversations blur them together in a way that leads to false confidence.
HCG on TRT: What It Can and Cannot Do
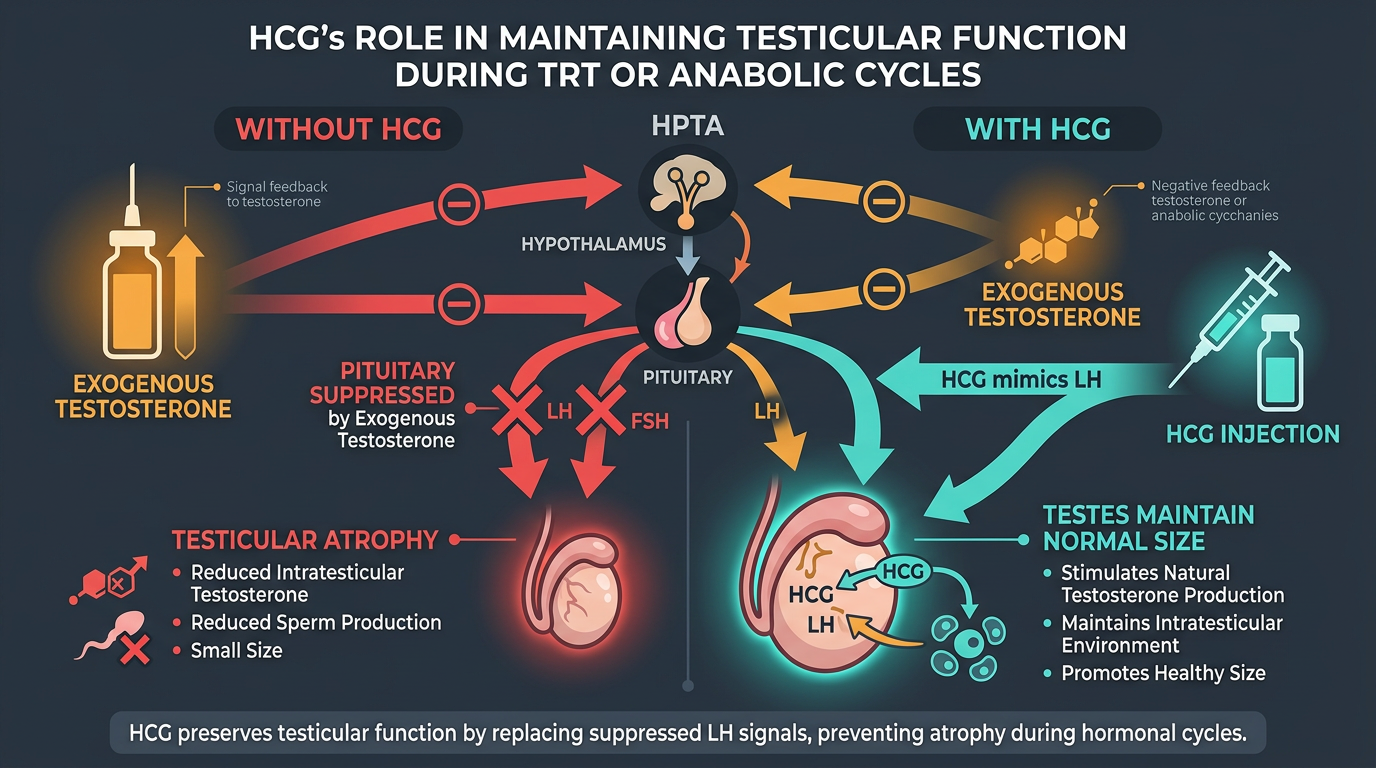
Human chorionic gonadotropin (HCG) acts on the same testicular receptors as LH and essentially replaces part of the LH signal that exogenous testosterone suppresses. That is why HCG is commonly used in fertility-conscious TRT management. Its role is straightforward: keep the testes receiving enough stimulation that intratesticular function is better maintained than it would be on TRT alone.
Men who add HCG appropriately usually notice three things: less testicular atrophy, better preservation of testicular fullness, and a better chance of maintaining fertility potential. Some also report subjective improvements in libido or sense of wellbeing, though these experiences vary.
The important limitation is that HCG is not a fertility guarantee. It can help preserve function, but it does not recreate a fully normal endogenous reproductive axis. FSH signaling, baseline fertility, age, prior anabolic use, time spent suppressed, and individual biology all still matter. The right mental model is “risk reduction,” not “certainty.”
Testicular Atrophy and Ejaculate Volume
Many men notice TRT-related changes that are not dangerous but are still psychologically meaningful. The most common are testicular shrinkage and lower ejaculate volume. Both are directly related to reduced gonadotropin signaling and reduced internal testicular activity.
These changes matter because they often become the first obvious sign that TRT is not merely “adding testosterone on top” of a fully functioning natural system. It is replacing and suppressing. Some men are unbothered by this. Others find it distressing. Neither reaction is irrational. It is simply better to understand the change in advance than to interpret it as something going unexpectedly wrong.
Estrogen-Related Side Effects on TRT
TRT side-effect discussions often become too fixated on estradiol, but it is still a real variable. When dose or injection pattern produces higher peaks, some men experience water retention, nipple sensitivity, emotional lability, or a bloated look. These symptoms are often made worse by body-fat level, because adipose tissue expresses aromatase and increases the conversion of testosterone to estradiol.
Many TRT users assume every symptom remotely compatible with estrogen means they need an AI. In practice, protocol changes often solve the problem more cleanly: lowering a dose that is too high for true replacement, splitting injections more frequently, improving body composition, or simply giving the protocol enough time to stabilize.
Hair Loss and Skin Changes
Androgenic alopecia, male-pattern baldness, is genetically mediated. TRT does not create that predisposition out of nowhere, but it can accelerate the process in men who are already predisposed. Testosterone is converted to DHT by the 5AR enzyme in scalp follicles. In susceptible individuals, DHT progressively miniaturizes the follicle over time.
Acne and oilier skin can also occur, especially early in treatment or after aggressive dose increases. These usually reflect androgen sensitivity and peak exposure more than some mysterious incompatibility with TRT itself. The practical takeaway is simple: more testosterone exposure generally means more androgenic pressure on skin and hair. This is another reason not to treat TRT like a place to chase the highest possible dose.
Finasteride, a 5AR inhibitor, is commonly used for hair-loss management because it lowers DHT. It can be helpful, but it is not cost-free. Some users tolerate it well, others do not, and the decision to use it is best framed as a tradeoff rather than as a universally obvious move.
Hematocrit, Blood Pressure, and Polycythemia
Testosterone stimulates erythropoiesis through multiple pathways, including increased EPO signaling and direct effects on marrow activity. Over time, some TRT users develop rising hemoglobin and hematocrit. This matters because thicker blood places more strain on the cardiovascular system and raises thrombotic concern, particularly when combined with other issues like sleep apnea, dehydration, smoking, or uncontrolled blood pressure.
Hematocrit above roughly 52-54% deserves real attention. The correct response is not always the same. Sometimes the issue is simple dose excess. Sometimes the problem is long intervals between injections producing high peaks. Sometimes untreated sleep apnea is driving part of the red-cell response. Sometimes blood donation or therapeutic phlebotomy becomes part of the management picture. What matters is that rising hematocrit triggers evaluation rather than denial.
Blood pressure belongs in the same conversation. A man can feel “great on TRT” while quietly drifting into worse cardiovascular risk if blood pressure, hematocrit, and lipids are not being followed.
Mood, Libido, and Oversimplification
TRT can improve mood and libido substantially in genuinely hypogonadal men, but those effects are not linear forever. More is not always better. Some men feel worse on protocols that are too aggressive, too peaky, or too heavily managed with ancillaries. Irritability, emotional volatility, flat mood, libido decline, and sleep disruption can all appear when a protocol is poorly tuned.
Trying to explain every symptom with one hormone is where a lot of people go wrong. Libido problems may reflect low testosterone, high estradiol, low estradiol, stress, relationship strain, poor sleep, or unrealistic expectations. TRT is powerful, but it does not exempt a person from normal physiology and normal life variables.
Long-Term Cardiovascular Data: What We Can Say Honestly
The long-term TRT debate is full of overstatement in both directions. One side treats TRT as cardiovascular poison. The other treats it as obviously cardioprotective in every context. Neither is a serious summary of the evidence.
The TRAVERSE trial (2023), the largest randomized controlled trial of TRT, found that testosterone therapy did not significantly increase major adverse cardiac events compared with placebo in the studied population. That is important and reassuring. At the same time, it also found statistically significant increases in certain problems including atrial fibrillation, pulmonary embolism, and non-fatal arrhythmia. So the takeaway is not “TRT is risk-free.” The takeaway is that physiological replacement does not appear to create the kind of dramatic hard-event increase that critics once feared, but it still requires proper patient selection and real monitoring.
The men most likely to get into trouble are not the ones treating TRT like steady long-term medical therapy. They are the ones who drift from replacement into enhancement while continuing to use the reassuring language of medicine.
The Big Picture
TRT can be an excellent long-term therapy for the right patient, but it is not a free upgrade. It is a trade. The trade may be worth it, but it must be understood clearly: improved energy, libido, mood, body composition, and quality of life on one side; ongoing monitoring, fertility consequences, androgenic side effects, and chronic risk management on the other.
The men who do best on TRT are usually the ones who treat it with the least fantasy. They understand what it can improve, what it can suppress, what it cannot solve, and what must be monitored over time if they want the benefits without drifting into preventable harm.
Selected references for major clinical, mechanistic, or protocol claims. Community-practice points may not be cited individually.