Managing Estrogen on TRT
Why estrogen management is one of the most misunderstood aspects of TRT, when AI use is and isn't warranted, and how to avoid the common mistake of crashing your estradiol.
- Understand why testosterone aromatizes and what this means for TRT users
- Identify the optimal estradiol range for TRT and the consequences of levels outside that range
- Recognize when AI use is and isn't warranted
- Understand the pharmacological differences between Arimidex and Aromasin
- Explain how body fat and lifestyle influence aromatization on TRT
Estrogen on TRT
Few topics in TRT management generate more confusion than estrogen. The dominant narrative in many online TRT communities is that estrogen is testosterone’s enemy, a byproduct to be suppressed aggressively. This framing is directly responsible for one of the most common iatrogenic harms in the TRT-using population: crashed estradiol from overuse of aromatase inhibitors.
Estradiol is not a toxin. It is an essential hormone in the male body responsible for bone density maintenance, cardiovascular protection, cognitive function, mood regulation, joint lubrication, and sexual function. Men with no estrogen experience bone loss, joint pain, severe depression, and paradoxically, loss of libido and erectile dysfunction.
Why Testosterone Aromatizes
When exogenous Testosterone is introduced, the body metabolises a portion of it through aromatization, the conversion of androgens to estrogens via the aromatase enzyme. The primary aromatization sites are adipose (fat) tissue, the liver, and the brain. Adipose tissue is the most quantitatively significant: the more body fat a man carries, the more aromatase enzyme he expresses, and the more of his Testosterone dose is converted to estradiol. For many TRT users with elevated estradiol driven primarily by excess adiposity, weight loss is a more sustainable intervention than an AI.
What Is the Optimal Estradiol Range on TRT?
The sensitive estradiol assay (LC/MS-MS method) should be specified for men on TRT. On the sensitive assay, most practitioners find that symptoms of estrogen excess begin to appear above 50–70 pg/mL, while symptoms of estrogen deficiency begin below 15–20 pg/mL. The therapeutic sweet spot is generally 25–50 pg/mL, with individual variation. A number on a lab result is not an indication for treatment in isolation, a TRT user with estradiol of 55 pg/mL who is asymptomatic does not need an AI.
When AI Use Makes Sense
An AI is genuinely indicated in a small subset of TRT users: those with symptomatic high estradiol that does not resolve with lifestyle interventions or dose reduction. For isolated gynecomastia concerns on TRT, Tamoxifen at low doses (10–20 mg/day) blocks estrogen receptor activity in breast tissue without affecting systemic estradiol levels, often a more targeted tool than a systemic AI.
Arimidex and Aromasin: Pharmacological Differences
Arimidex (anastrozole) is a reversible, non-steroidal AI. That means it temporarily sits on the aromatase enzyme and blocks testosterone from being converted into estradiol, but it does not destroy the enzyme. Think of it like putting a cap on the machinery. While the drug is present, estrogen production is reduced. As the drug level falls, that same aromatase enzyme is available to start working again. On TRT, that makes anastrozole easier to titrate in small adjustments, but it also means estrogen can swing back up when the drug wears off because the enzyme pool is still there waiting. Dosing in TRT context is typically 0.25–0.5 mg taken once or twice weekly. A critical concern is that its metabolism is strongly influenced by CYP2C19 polymorphisms, some people metabolize it much more slowly, making them highly prone to estrogen suppression at doses that are fine for others.
Aromasin (exemestane) is a steroidal, irreversible AI. It is often called a “suicide inhibitor,” and that phrase sounds dramatic but the meaning is simple: the drug binds to aromatase, the enzyme tries to process it as a normal substrate, and in the process that specific enzyme molecule is permanently inactivated. In other words, the enzyme is not just paused, it is taken out of service. Estradiol does not recover until your body builds new aromatase enzyme. On TRT, that usually means exemestane produces a smoother fall in estrogen rebound when stopped, because there is no intact blocked enzyme suddenly coming back online all at once. The tradeoff is that if you overshoot and crash estrogen, recovery is not as simple as waiting for today’s dose to wear off, you have to wait for new enzyme production. That is why people often describe Aromasin as more stable but less forgiving if you dose too aggressively.
Crashing Estrogen
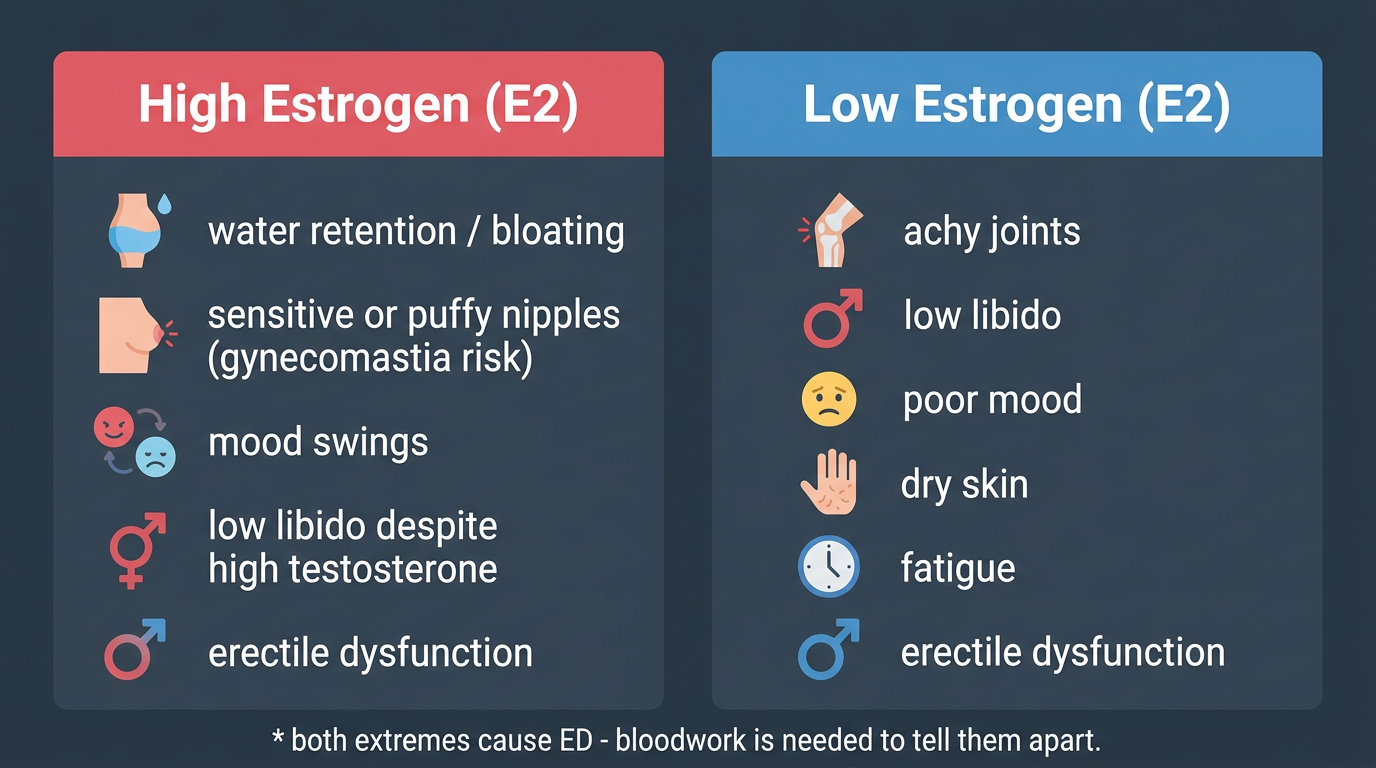
Many TRT users do the same thing. They see mild water retention, a slightly high estradiol number, or a vague sense of bloating, then overcorrect with an AI and feel dramatically worse. Joint pain is one of the earliest and most consistent signs of estradiol deficiency. The synovial environment that keeps joints moving comfortably depends in part on estrogenic signaling; men with very low estradiol often feel dry, stiff, and beaten up for reasons they mistakenly blame on training.
Libido and erectile function frequently suffer more from low estradiol than from mildly elevated estradiol. Mood effects can also be severe: dysphoria, emotional blunting, anxiety, irritability, and a flat affective tone. In real TRT practice, mildly high estrogen is often less destructive than aggressively low estrogen. The man who is a little puffy but otherwise feels good usually needs better context, not an aggressive correction. The man who has crashed estrogen often feels like his whole system stopped working at once.
Selected references for major clinical, mechanistic, or protocol claims. Community-practice points may not be cited individually.