TRT Protocols: Dosing, Frequency, and Delivery Methods
A practical guide to the different forms of testosterone used in TRT, how dosing and injection frequency affect hormonal stability, and the trade-offs between injectable, topical, and implant-based delivery.
- Understand the main testosterone formulations used in TRT and their pharmacokinetic differences
- Explain how injection frequency affects hormonal stability and downstream side effects
- Compare subcutaneous and intramuscular injection routes for TRT
- Evaluate the trade-offs of topical, pellet, and injectable delivery methods
The Pharmacokinetic Foundation of TRT Protocol Design
Every TRT protocol is fundamentally a pharmacokinetic problem. You are not just “taking testosterone.” You are trying to deliver exogenous Testosterone in a pattern that approximates a stable, physiologically appropriate hormonal environment. If the dose is technically reasonable but the delivery pattern produces extreme peaks and troughs, the user may still end up with avoidable problems: mood volatility, excessive aromatization, injection-day highs followed by end-of-week crashes, and labs that are harder to interpret cleanly.
Understanding the concept of an ester is essential before discussing specific formulations. In pharmaceutical chemistry, an ester is a chemical modification attached to the base testosterone molecule that slows its release from the injection depot into the bloodstream. The longer the ester chain, the slower the release, the longer the half-life, and the more spacing flexibility you have between injections. Protocol design is therefore not just a dose question. Timing matters too.
The Goal of a Good TRT Protocol
A good TRT protocol should do four things at the same time:
- Restore testosterone to a physiological range.
- Keep symptoms improved across the full week, not just for 24 hours after an injection.
- Minimize secondary problems like excessive estradiol swings, hematocrit creep, and mood instability.
- Be simple enough that the patient can actually follow it consistently for years.
This last point matters more than people think. A protocol that looks perfect on paper but is too inconvenient to maintain is not a good long-term protocol. TRT is chronic therapy, so practical adherence matters almost as much as pharmacology.
Testosterone Formulations Used in TRT
Testosterone Cypionate is the most commonly prescribed injectable testosterone in the United States. It has an ester that confers a half-life of approximately 8 days in most individuals. Its relatively long half-life allows weekly, twice-weekly, or even more frequent split dosing without the dramatic instability seen with shorter-acting preparations. Many clinics start here because it is familiar, widely available, and predictable.
Testosterone Enanthate is functionally very similar to Cypionate, with a half-life of approximately 7-8 days. It is the most widely used injectable testosterone globally outside the United States. For TRT purposes, Enanthate and Cypionate are largely interchangeable. Most users will not “feel” a meaningful difference between them if the total weekly dose and injection schedule are equivalent.
Testosterone Propionate carries a much shorter ester, with a half-life of only 2-3 days. This means Propionate usually requires ED or EOD administration to maintain stable levels. That can work, but for most TRT patients it adds hassle without adding much therapeutic value. Propionate is better understood as a niche option than a standard TRT foundation.
Some regions also use long-acting undecanoate preparations, which dramatically reduce injection frequency. These are convenient for some patients, but they also reduce flexibility. If the dose is too high, if hematocrit climbs, if side effects develop, or if the patient simply feels wrong on the protocol, you cannot make quick adjustments the way you can with Cypionate or Enanthate.
Typical Dosing Ranges for TRT
In a clinical TRT context, focused on restoration rather than enhancement, the typical weekly dose of injectable Testosterone falls somewhere around 100-200 mg per week. The prescribing goal is to achieve total testosterone levels in the mid-to-upper physiological range, often roughly 500-900 ng/dL depending on symptoms, SHBG, free testosterone, timing of labs, and provider philosophy.
The number of milligrams is not the target. The hormonal outcome is. One man may feel and test well on 100 mg/week. Another may require meaningfully more to land in the same physiological zone. That is one reason protocol conversations that focus only on weekly milligrams become misleading so quickly. Dose response is individual, and good TRT management is built around symptoms plus labs, not around internet dosage folklore.
Doses materially above 200 mg/week begin to push many men out of replacement territory and into supraphysiological territory. That does not mean every man on 210 mg/week is “blasting.” It does mean that the farther a protocol gets from physiological lab outcomes and symptom-driven care, the less honest it is to describe it as pure replacement.
Injection Frequency and Hormonal Stability
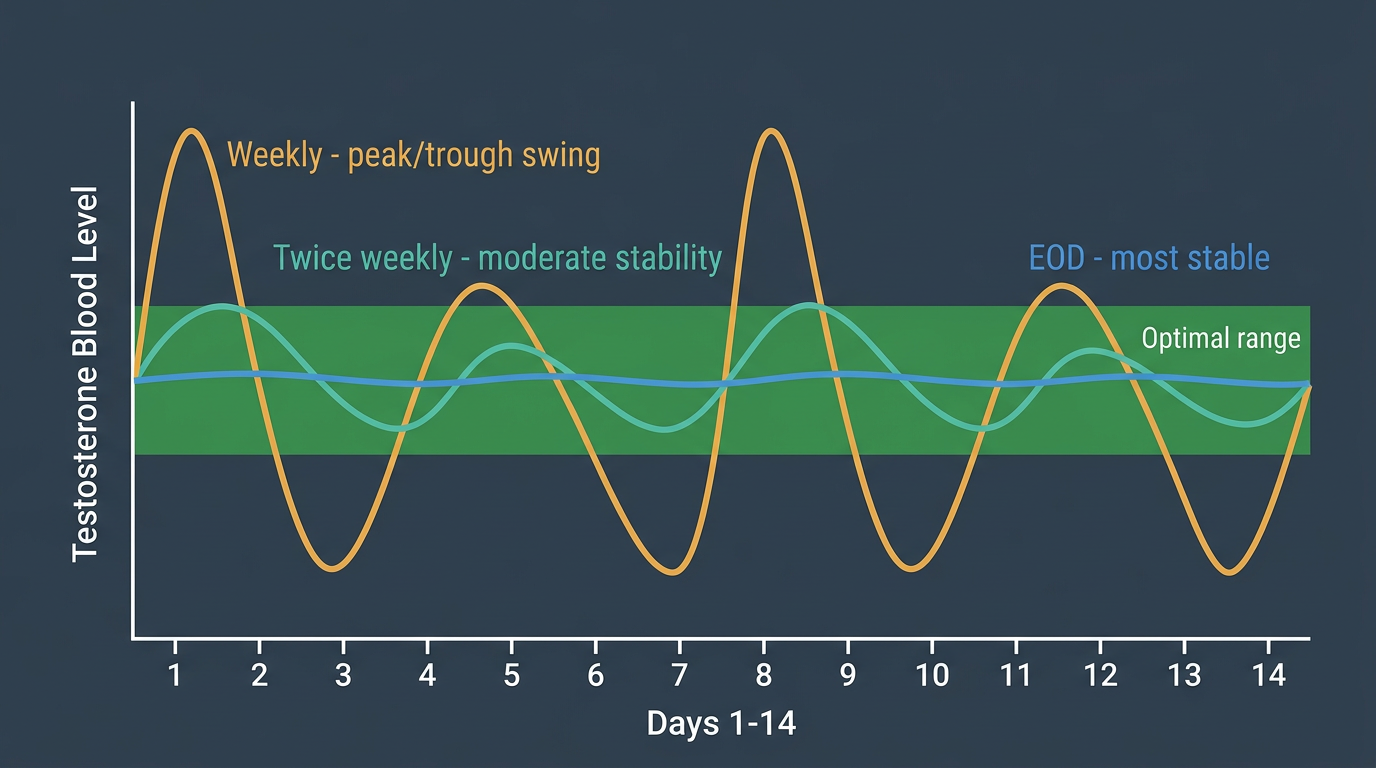
One of the most practically important decisions in TRT protocol design is how often to inject. With a long-ester compound like Cypionate or Enanthate, a single weekly injection can work, but it often produces a noticeable trough-to-peak swing. Testosterone rises after the shot, aromatization rises with it, then levels drift downward over the week. Some men tolerate that just fine. Others feel it clearly.
The men who notice poor response to once-weekly injections often describe the same pattern: they feel strong or stimulated early in the week, then flatter, more fatigued, or more emotionally off toward the end. Some also see more estrogen-related symptoms at the peak because aromatization tends to track serum testosterone concentration. Higher peaks mean more substrate available for conversion to estradiol.
Splitting the same weekly dose into two injections, or sometimes into even smaller, more frequent administrations, often smooths this out. The total weekly amount is unchanged, but the hormonal curve is flatter. That often means fewer mood swings, less nipple sensitivity, less water retention, and a more stable overall sense of wellbeing. For that reason, frequency changes are often a better first intervention than immediately adding an AI.
Common TRT Injection Schedules in Practice
Several patterns are commonly used:
- Once weekly: simplest, but most likely to produce peaks and troughs in sensitive patients.
- Twice weekly: a very common compromise between convenience and stability.
- Every 3.5 days or E3D: often used by patients who want tighter stability without daily injections.
- Daily microdosing: sometimes helpful in very sensitive patients, though it adds complexity and is not automatically superior.
The best schedule is usually the simplest one that gives stable symptoms, interpretable labs, and good adherence.
Subcutaneous vs. Intramuscular Injection for TRT
Subcutaneous injection, into the fatty tissue just beneath the skin, is increasingly common in TRT because it works well at standard doses and smaller volumes. It offers several practical advantages: easier self-administration, shorter finer needles, less PIP, and a lower psychological barrier for patients who dislike deep injections. Many men find it much easier to stay compliant long-term with subcutaneous dosing.
Intramuscular injection remains completely appropriate and, in some settings, still the default. It may be preferable when larger volumes are being administered, when the patient is already comfortable with IM technique, or when body composition makes subcutaneous absorption less predictable. In real practice, both routes can work well. The decision is less about ideology and more about comfort, consistency, and how the patient responds.
A common mistake is treating route choice as a tribal identity issue. It is not. If labs are stable, symptoms are good, and the patient can perform the injections reliably and safely, the route is doing its job.
Non-Injectable Delivery Methods
Not every TRT patient wants injections, and injections are not the only option.
Topical gels and creams allow needleless administration and are appealing to patients who want a simple daily routine. Their main weaknesses are variable absorption, daily compliance demands, and the risk of skin transfer to partners or children. That transfer risk is not a trivial footnote; it is a real practical limitation in family settings.
Patches offer more consistent dosing than many topical gels, but skin irritation is common enough that they are often abandoned.
Pellets provide months of convenience after a minor implant procedure. For some patients this is excellent. For others it is frustrating because it removes flexibility. If the dose is wrong, if symptoms are not improving, or if side effects develop, you cannot simply adjust next week’s dose.
The tradeoff across all non-injectable options is the same: less injection burden, but usually less control.
How Protocols Get Adjusted
Good TRT management rarely involves dramatic changes. Most protocol refinement happens in small steps. If the patient feels underdosed and labs confirm low trough levels, the dose may need to rise. If estradiol symptoms are appearing around peaks, frequency may need to increase before adding any ancillary medication. If hematocrit is climbing, the clinician may reduce dose, adjust frequency, evaluate hydration and sleep apnea, and look at broader cardiovascular risk rather than treating the lab number in isolation.
This is another place where internet advice often goes wrong. Many users see every TRT issue as a drug-deficiency problem to solve by adding more compounds or more interventions. In reality, many TRT problems are protocol-shape problems, not raw-dose problems. The user may not need more testosterone. He may need the same amount delivered in a better pattern.
Common Protocol Mistakes
The most common TRT protocol mistakes are predictable:
- Starting too high because the patient wants to “feel it.”
- Interpreting short-term stimulation as therapeutic success.
- Making adjustments before steady-state has been reached.
- Using an AI before fixing dose and frequency.
- Copying a bodybuilding-style protocol and calling it TRT.
A TRT protocol should feel boring in the best possible way. Stable energy, stable libido, stable mood, and stable labs are the win. When the protocol is constantly being chased, tweaked, and rescued with ancillaries, that usually means the foundation was not built correctly.
Selected references for major clinical, mechanistic, or protocol claims. Community-practice points may not be cited individually.