Hormones, the HPTA, and Suppression
How the hypothalamic-pituitary-testicular axis works, why exogenous androgens suppress it, and what recovery requires.
- Describe the hypothalamic-pituitary-testicular axis and its feedback loops
- Explain how and why exogenous androgens cause HPTA suppression
- Understand LH, FSH, and their roles during and after a cycle
- Identify factors that affect HPTA recovery timeline and the risks of permanent suppression
The Hormonal System You Are Disrupting
Before discussing how exogenous androgens alter the endocrine system, it is essential to understand the system as it exists in a healthy male. The HPTA, the Hypothalamic-Pituitary-Testicular Axis, is an elegant negative-feedback loop that regulates testosterone production with remarkable precision across an enormous range of physiological conditions.
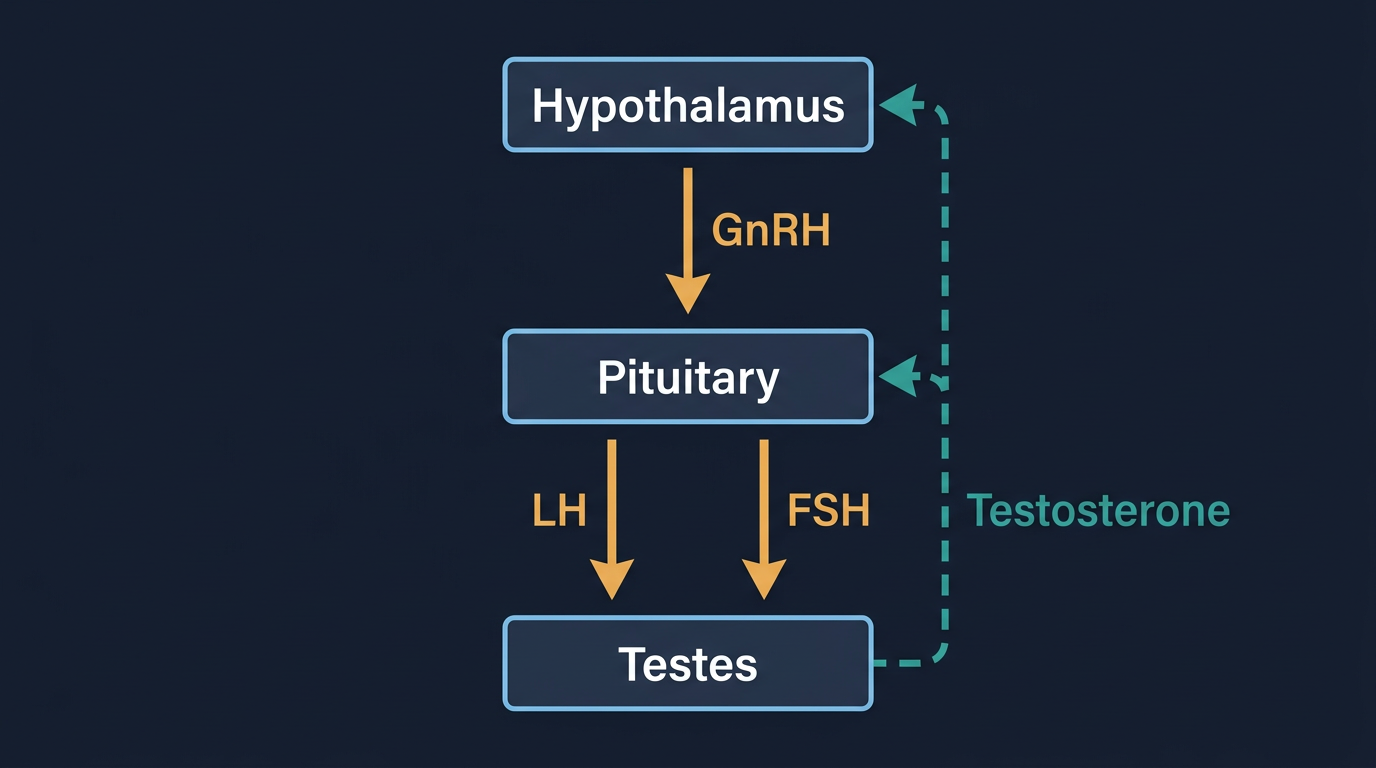
The cascade begins in the hypothalamus, a small region at the base of the brain that secretes gonadotropin-releasing hormone (GnRH) in short, pulsatile bursts roughly every 60–90 minutes. These GnRH pulses travel to the anterior pituitary gland, where they stimulate the synthesis and release of two key hormones: LH (Luteinizing Hormone) and FSH (Follicle-Stimulating Hormone).
LH travels in the bloodstream to the Leydig cells of the testes, where it binds to receptors and triggers the production and secretion of testosterone. This LH-to-testosterone signal is the primary driver of testicular testosterone output. FSH, in parallel, acts on the Sertoli cells of the testes to support spermatogenesis, the production of sperm. Healthy sperm production requires both FSH signalling and adequate intratesticular testosterone concentrations (which are roughly 50–100× higher inside the testes than in peripheral blood).
The feedback mechanism that closes the loop is elegant in its simplicity: when testosterone (and its metabolite estradiol) rises above a threshold in the bloodstream, it signals both the hypothalamus and the pituitary to reduce GnRH, LH, and FSH output. When testosterone falls, the brake is released and output increases. This self-regulating system maintains circulating testosterone within a relatively narrow physiological band, roughly 300–1000 ng/dL in healthy adult males, with morning peaks and evening troughs.
How Exogenous Androgens Suppress the HPTA
When you introduce an exogenous androgen, Testosterone Enanthate, Nandrolone Decanoate, Trenbolone Acetate, or any other anabolic compound, you are flooding this feedback system with a hormonal signal that it interprets as excess production. The hypothalamus senses circulating androgen (and in the case of aromatizing compounds, circulating estradiol) above the normal threshold and responds by reducing or eliminating GnRH pulsatility. Without GnRH pulses, the pituitary stops releasing LH and FSH. Without LH, the Leydig cells stop producing testosterone. Without intratesticular testosterone and FSH, spermatogenesis slows to a halt.
This is suppression, and suppression is a direct, predictable, mechanistically inevitable consequence of exogenous androgen use, not a side effect in the colloquial sense. Every compound that activates androgen receptors or aromatizes to oestrogen will suppress the HPTA to some degree. The questions are how fast, how complete, and how reversible the suppression is.
For most anabolic compounds, suppression of LH and FSH to near-zero occurs within 2–4 weeks of use at supraphysiological doses. Testicular atrophy (a reduction in testicular volume due to loss of LH-dependent Leydig cell activity and reduced intratesticular fluid) follows over weeks to months of continued use. This is the visible, tactile manifestation of HPTA shutdown, a normal physiological adaptation to sustained exogenous hormone input, not a sign of permanent damage.
The depth and rapidity of suppression varies by compound and dose. Nandrolone (particularly its Decanoate ester, commonly known as Deca) is notable for causing very deep and prolonged suppression that can be significantly harder to recover from than that caused by Testosterone alone. Part of this relates to its progestogenic activity, [Nandrolone] activates progesterone receptors in the hypothalamus and pituitary, adding a second suppressive signal on top of the androgen-receptor-mediated pathway. Similarly, Trenbolone, which is neither aromatizing nor a potent progesterone agonist in the traditional sense but is an extraordinarily potent androgen, causes rapid and deep HPTA suppression that many users find difficult to recover from.
The Role of LH and FSH During and After a Cycle
During a cycle, LH and FSH at or near zero in a blood panel is expected and does not itself represent a problem. The testes are effectively in standby mode, not needed while exogenous hormone supply is circulating. Some users choose to include human chorionic gonadotropin (hCG) during longer cycles to maintain Leydig cell responsiveness and prevent the degree of testicular atrophy that develops during prolonged suppression. hCG mimics LH at the Leydig cell receptor and keeps the testes producing intratesticular testosterone even in the absence of pituitary LH. For short cycles under 12–14 weeks the need is debated, but most practitioners consider it best practice for longer durations or bridges between cycles.
Post-cycle, the recovery of LH and FSH is the biological signal that the HPTA is restarting. The timeline is not fixed, it depends on the compounds used, the duration of use, the doses, individual variability in hypothalamic sensitivity, and whether PCT medications are used. In the absence of PCT, recovery of measurable LH and FSH typically begins 2–6 weeks after the last injection (accounting for ester clearance) and full recovery of normal endogenous total testosterone takes 3–6 months in typical cases.
PCT protocols using SERMs, Tamoxifen (Nolvadex) and Clomiphene (Clomid), work by competitively blocking oestrogen receptors in the hypothalamus and pituitary. By blocking the oestrogen-mediated negative feedback, they effectively remove the brake on GnRH and LH/FSH secretion, accelerating the restart of the axis. They are therefore used at the start of PCT, after exogenous compounds have largely cleared from the system. Starting PCT while long-ester compounds are still highly active in circulation is a common error, the ongoing exogenous androgen presence continues to suppress the axis regardless of the SERM, rendering the PCT ineffective.
Factors That Affect Recovery Timeline
Recovery of the HPTA is not automatic or guaranteed, and several factors meaningfully modulate its timeline and completeness:
Duration of use. The longer the HPTA has been suppressed, the more time it requires to restart. The axis can downregulate receptor sensitivity and reduce GnRH pulse generator activity over time. Cycles under 12 weeks from fully suppressing compounds typically recover more readily than cycles exceeding 20+ weeks.
Compound selection. As discussed above, 19-nor compounds (Nandrolone, Trenbolone, Trestolone) are associated with more difficult recovery than testosterone-based cycles. Trenbolone in particular has a reputation for prolonged post-cycle dysfunction, likely due to its potency at the androgen receptor and possible direct effects on hypothalamic function.
Age. Recovery capacity is strongly correlated with age. Users in their mid-twenties typically recover faster and more completely than users in their forties. This is likely related to age-related decline in Leydig cell number and responsiveness independent of cycle history.
Baseline HPTA health. Users with pre-existing subclinical hypogonadism (borderline low total testosterone at baseline) are more vulnerable to prolonged or incomplete recovery, since the HPTA has less functional reserve to draw on.
Blast and cruise patterns. Users who move continuously between cycles without ever allowing recovery, the blast and cruise approach, may never give the HPTA the sustained absence of exogenous signal it needs to restart. Over years, this can transition from a temporary suppressed state to a functional state where endogenous production no longer meaningfully recovers, making TRT or continued exogenous management a long-term or permanent commitment.
The Cost of Permanent Suppression
Permanent or chronic HPTA dysfunction, whether from years of heavy, sustained blast and cruise use, from particularly difficult recovery scenarios, or from individual vulnerability, has real physiological consequences that extend beyond simply needing exogenous hormone replacement.
The testes serve endocrine functions beyond testosterone production. Adequate intratesticular hormonal environment supports spermatogenesis, and permanent impairment of FSH-driven Sertoli cell function can result in lasting or irreversible infertility. The recovery of spermatogenesis typically lags behind the recovery of testosterone production, and for some users on prolonged protocols involving deep FSH suppression, particularly those involving Nandrolone Decanoate, fertility recovery may require FSH supplementation (recombinant FSH) or prolonged hCG therapy.
Beyond fertility, the ongoing low-testosterone state that characterises poor recovery carries its own health burden: reduced bone mineral density, increased visceral adiposity, reduced protein synthesis and lean mass, mood disturbances, and reduced cardiovascular function. These are not abstract risks, they are the clinical profile of hypogonadism, which has an established literature on morbidity.
For users who have committed to a long-term blast and cruise lifestyle and for whom natural recovery is no longer a practical expectation, medically supervised TRT provides a stable and manageable alternative. It is a permanent medical commitment with ongoing monitoring requirements that carries its own considerations around fertility, hematocrit management, and lipid health that should be entered into deliberately rather than by default.
Managing the HPTA Sensibly
The practical lessons from understanding the HPTA are direct: keep cycle durations reasonable, allow adequate time off for recovery, consider hCG for longer cycles, plan PCT appropriately and time it correctly, monitor LH, FSH, and total testosterone post-cycle to confirm recovery, and treat persistent suppression as a medical issue requiring professional evaluation rather than as a problem to self-manage indefinitely.
The HPTA is not infinitely resilient. It can tolerate episodic disruption with thoughtful management, but it has limits, and those limits vary between individuals in ways that make population-level assumptions about your personal recovery unreliable. Your bloodwork is the only honest feedback mechanism you have.
Selected references for major clinical, mechanistic, or protocol claims. Community-practice points may not be cited individually.